|
|
Case Reports Indian Pediatrics 2000;37: 1134-1137 |
|||||||
|
Neonatal Pharyngeal Pseudo-Diverticulum |
|||||||
|
Y.K. Sarin D. Goel N.B. Mathur* A. Maria*
Accidental perforation of the esophagus and hypopharynx occurs rarely in newborn infants(1-3). The risk of misdiagnosing these perforations as esophageal atresia is quite high as clinical presentation is similar(4,5). This is important, as the management of these perforations is largely conservative, whereas esophageal atresia will require operative correction. Early clues to the diagnosis of pharyngo-esophageal perforation may be subtle but should be looked for before instituting the specific treatment. In this report, we present an unusual case of neonatal pharyngo-esophageal perforation resulting in pharyngeal pseudo-diverticulum, which required operative intervention.
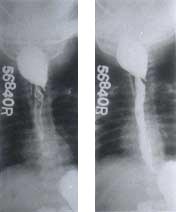
A full-term, 21-day-old female neonate, weighing 3 kg, was admitted to the Referral Nursery of Department of Pediatrics with complaints of excessive salivation and inability to feed for eight days. The baby had been feeding well till the 11th day of life. On repeated questioning, the mother recalled some degree of salivation since birth. The pregnancy was uncomplicated and the vaginal delivery was conducted at home by traditional untrained birth-attendant. There was no history of endotracheal or nasogastric intubations. A clinical diagnosis of pharyngeal pseudo-diverti-culum was made. With a little manoeuvring, a nasogastric tube could be passed in the stomach and the nasogastric feeds were initiated. The neonate required very frequent suctioning to clear the oropharynx of secretions. Esophagography performed after two weeks revealed pharyngeal pseudo-diverticulum; the dye passed freely into the stomach (Fig. 1). The child continued to have excessive salivation even at four weeks of expectant management. At this stage, differen-tial diagnosis of a true pharyngeal diverticu-lum was entertained. A true diverticulum is not expected to resolve with expectant therapy as against a pseudo-diverticulum, which has been known to resolve in 7 to 10 days. Esophago-scopy could not differentiate whether it was a true or a pseudo-diverticulum. A cervical exploration was then undertaken; it revealed pharyngeal pseudo-diverticulum and a 3 cm long longitudinal perforation in the region of pharyngo-esophageal junction, which was repaired in single layer using interrupted 5.0, polyglactin sutures. The infant had a stormy post-operative period including a minor salivary leak, which healed spontaneously. The oral secretions subsided slowly. A repeat esophagography performed three weeks post-operatively revealed normal esophageal anatomy. The infant was discharged after two months of hospitalization and has been doing well on follow-up.
Eklof first reported perforation of the hypopharynx or cervical esophagus in a newborn caused by an aspiration catheter in 1968(6). Since then, case reports have appeared in the literature describing the etiological factors, the clinical features and the management of neonatal pharyngo-esophageal perfora-tions(3,5). These perforations can be divided into iatrogenic and non-iatrogenic. Non-iatrogenic perforations are extremely rare, and usually occur at the lower end of the esophagus(7). latrogenic perforations, more commonly seen in small for gestational age and premature babies, usually occur in the cervical esophagus at the level of cricopharyngeus muscle(3,4). The esophageal lumen is narrowest at this point and may get occluded by spasm or reflex constriction of the cricopharyngeus in response to injury or an offending agent(2). The mechanism of injury is believed to be resuscitative measures undertaken in the neonatal nursery, and rarely, the insertion of the obstetrician’s finger into the oral cavity of the after-coming head in breech presentation(1,3,8).
The clinical presentation of neonatal pharyngo-esophageal perforations could vary(3). When there is either a submucosal tear, or the leak is confined to the mediastinum, the condition mimics esophageal atresia. There is excessive drooling of saliva from the mouth, feeding difficulties secondary to the cricopharyngeal spasm, failure to pass a nasogastric tube into the stomach and respiratory difficulty(2,4,9). There are, however, a few subtle differences in presentation, which may clinch the diagnosis. Unlike esophageal atresia, there would be no history of maternal polyhydramnios. The late presentation such as on 10-14 day of life, as seen in our case is usually not compatible with the diagnosis of esophageal atresia. In pharyngo-esophageal perforations, blood stained secretions may be obtained on suctioning of the oral cavity, a feature rarely seen at presentation in patients with esophageal atresia(4). The second group of infants have a free perforation into the pleural cavity, usually the right(1), with resultant pneumothorax or pyopneumothorax(10). These patients rapidly develop severe respiratory symptoms and a prompt intervention is important. The radiological features are often subtle and need to be carefuuly studied. Retropharyngeal or subcutaneous air may be seen on plain films of the neck(8). Pneumomediastinum, pneumothorax or an air fluid level in the chest may be present(4). The position and course of the nasogastric tube may be diagnostic(8). The nasogastric tube unable to bypass the cricopharyngeal spasm may coil in the neck mimicking esophageal atresia. The nasogastric tube may course through the perforation and burrow alongside the esophagus, only to get arrested at the level of the domes of the diaphragm bending to one or the other side(4,5). Lastly, the nasogastric tube may sometimes overcome the cricopharyngeal spasm and pass unimpeded into the stomach avoiding the site of the perforation(8), as happened in our patient. The diagnosis of pharyngo-esophageal perforation can be confirmed by careful contrast esophagography using water-soluble contrast(10). This study may demonstrate three varying degrees of injury: firstly, a pharyngeal pseudo-diverticulum created by a local cervical leak; second, a mucosal perforation extending posterior and parallel to the esophagus; and third, a free intrapleural perforation with spillage of the dye into the pleural cavity(10). Even after contrast esophagography, it may be occasionally difficult to differentiate this condition from esophageal atresia, associated cricopharyngeal muscle spasm may prevent passage of the dye beyond the upper esophagus or, filling up of a pseudodiverticulum alone may also simulate esophageal atresia(5). Esophagoscopy for diagnosing neonatal acute pharyngo-esophageal injuries and perforations has not been found to be useful; it may actually increase the size of the perforation(4). We performed esophagoscopy in our case as we had entertained a differential diagnosis of true esophageal diverticulum; this very rare condition also occurs posteriorly at the pharyngo-esophageal junction(11). It does not heal on conservative management and requires a surgical resection. Most authors agree that esophageal perforations in newborn can be managed conservatively with survival rates approaching 100%(3,4,5,8,10). A nasogastric tube may be negotiated into the stomach under fluoroscopic control and naso-gastric feedings begun. Failure of this procedure warrants parenteral nutrition or a feeding gastrostomy. Drainage of the neck or mediastinum is seldom required. An oral contrast study is performed after 7-10 days and oral feedings are started once healing of the esophagus is demonstrated. We feel that at times, it may take much longer than the usually quoted 10 days before child could be put on breastfeeds. We recommended operative closure in a rare case of pseudo-diverticulum, which does not heal on 2 to 3 weeks of expectant therapy. Esophageal dysmotility states may need to be ruled out in such patients on follow-up. The child reported here was delivered at home by untrained birth attendant and did not undergo any resuscitation or nasogastric intubations. We presume that the injury was caused by the birth attendant's finger while sweeping clear the oropharyngeal cavity of amniotic fluid, debris and mucus. Contributors: YKS was involved in the diagnostic analysis and interpretation of the case; he drafted the case report. NBM critically revised the manuscript; he was also involved in the diagnostic anlaysis and interpretation of the case. DG and AM helped in drafting the case report. Funding:
None.
|
![]()