|
|
Case Reports Indian Pediatrics 2000;37: 1117-1121 |
|||||||||||||
|
Neuromyelitis Optica with Transient Autonomic Disturbances |
|||||||||||||
|
Radhika H. Muzumdar Surekha Joshi Sushma Malik Sonali J. Tank Bina Easow
Devic’s disease (Neuromyelitis optica, Devic’s syndrome) is a rare disorder in pediatric age group and is characterized by acute or subacute optic neuritis and transverse myelitis (1-3). Neuromyelitis optica may present as an initial manifestation of multiple sclerosis, acute demyelinating encephalomyelitis (ADEM), SLE or Behcet’s disease. Autonomic disturbances are rare in association with Devic’s disease. Here we report a case of Devic’s disease in an 11-year-old boy who had autonomic disturbances and had clinical recovery with high dose methyl prednisolone therapy.
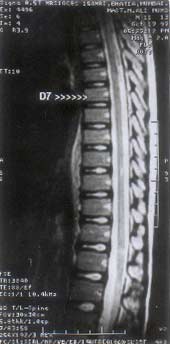
An 11-year-old boy presented to us with complaints of weakness of the lower extremities, inability to initiate voiding and diminished vision in the left eye of two days duration. He had low grade fever, pain and tingling in the lower extremities for one day prior to the onset of weakness. There was no history of prolonged fever, diarrhea, skin rash, recent immunization, radiating pain, back pain or trauma. General examination, including vital parameters (pulse - 76/min, respiratory rate - 24/min and blood pressure - 100/70 mmHg) were essentially normal. Cardiovascular system was normal and there was no organomegaly documented. CNS examination revealed paraparesis (Grade 1) with brisk tendon reflexes and extensor plantars. There were no meningeal signs, evidence of raised ICT, sensory levels or zone of hyperaesthesia and spine examination was normal. There was Marcus Gunn pupil in the left eye with diminshed vision (6/60). Fundus examination revealed that in the left eye, the disc was hyperemic and elevated with blurring of the disc margins which was suggestive of retrobulbar neuritis. In view of the above clinical findings, a diagnosis of transverse myelitis with left retrobulbar neuritis was made and possibility of Neuromyelitis optica was entertained. Routine investigations including CBC, ESR and chest X-ray were normal and Mantoux test was negative. CSF analysis showed proteins of 20 mg%, no cells and negative oligoclonal bands. Magnetic resonance imaging (MRI) of the brain and the spinal cord showed demyelination in left optic nerve, cervical segments C-2,3,4 thoracic D2-4, D10-12 segments and in conus medullaris (Figs. 1 & 2) There was a single subcortical white matter lesion documented in the frontoparietal region. Visual evoked potential (VEP) showed delayed conduction in the left optic nerve and somatosensory evoked potential (SSEP) documented absent conduction from the left tibial nerve. To rule out other underlying etiologies, ANA, dsDNA, color doppler and 2D Echo were done, and all were normal. Thus other causes for such type of presentations were excluded and the diagnosis of Neuromyelitis optica was confirmed.
The patient was started on intravenous methyl prednisolone (IVMP) therapy. The regime used was IVMP 250 mg every 6 hourly for 3 days, followed by oral prednisolone 1 mg/kg/day for eleven days. A short oral taper consisting of 20 mg on day 15 and 10 mg on days 16-18 was given. On the first day of therapy, patient developed diminished vision in the right eye (visual field constriction with paracentral scotoma) and autonomic disturbances in the form of fall in blood pressure, tachycardia and excessive sweating. These autonomic disturbances were transient and lasted for 48 hours. The patient responded well to the above regime of methyl prednisolone and showed almost complete recovery of power and substantial improvement in vision within 10 days. However, bladder retention persisted for three weeks. This necessiated intermittent catheterization and antibiotics for urinary infection. Repeat MRI done 6 weeks later showed improvement in all the lesions and there was no fresh lesions (Fig. 3). At 3 months follow up, eye examination showed a complete recovery with normal perimetry and color vision.
Albutt in 1920 was the first to recognize the association between spinal cord disease and blindness(1) whereas Eugene Devic's student Fernand Gault labelled it as neuromyelitis optica. Neuromyelitis optica is a clinical syndrome characterized by: (a) an acute or subacute onset, (b) involvement of both optic nerves and spinal cord, and (c) an interval between spinal cord involvement and optic nerve not exceeding one month(4). Such a combination of signs can be seen in multiple sclerosis or in various demyelinating disorders including diffuse sclerosis, post infectious and postvaccinal encephalomyelitis and acute disseminated encephalomyelitis(1-3). Specific associations with diseases such as SLE, varicella, tuberculosis and post viral infections have also been reported(5) though in most patients there is no identifiable specific etiology. Devic’s disease can occur in any age group from 5-66 years, but it is uncommon in pediatric age group. It usually presents with acute transverse myelitis with patchy or total sensory loss and visual symptoms. A history of flu, sore throat, myalgia may be seen in one third of cases. Visual loss may precede, occur simultaneously or follow the motor symptoms. In 40% of patients vision is affected acutely and eventually bilateral involvement occurs in 85%. Near complete visual loss, color blindness, bilateral hemianopia, generalized field constriction with central or paracentral scotomas, uveitis, anterior disc edema and Horner’s syndrome are some of the visual defects reported(1,6). Our patient had near complete visual loss in the left eye and field constriction with paracentral scotoma in the right eye. Autonomic disturbances though rare in Devic’s disease, can manifest as hypotension, rhythm disturbances, Horner’s syndrome and bladder dysfuction. Pathological changes reported in clinically typical Devic’s disease include white matter plaques, demyelination with vascular infiltrates, necrosis or cystic degeneration(1,7). Patients presenting with documented necrosis on neuroimaging, have a poorer prognosis for recovery. CSF findings are variable in this condition but in some cases consist of polymorphonuclear pleocytosis and increase in the protein content. In a series of 12 cases, Riordan et al.(5) demonstrated abnormal CSF in the form of neutrophil pleocytosis and oligoclonal bands in 16% of patients with Devic’s disease. Cock et al. have suggested that Devic’s syndrome may be distinct from multiple sclerosis as CNS IgG synthesis and oligoclonal bands are uncommon in the former(1,7) Somatosensory evoked potential and visual evoked potentials suggest it to be a demyelination process. The presentation in our patient corresponded to the sites of demyelination seen on MRI except the single subcortical lesion, which was clinically silent. Normal brain MRI has been one of the basis for some study groups to consider Devic’s disease distinct from multiple sclerosis(1,7). However, abnormal brain MRI has been demonstrated in 42% of patients with Devic’s in a series(5). The lesions are supratentorial and located in the frontoparietal white matter and tend to show partial resolution and absence of new lesions on follow up MRI, which is an unlikely pattern for multiple sclerosis. Lesions in multiple sclerosis tend to be periventricular in 90% of patients. In acute disseminated encephalomyelitis, the sites of demyelination tend to be smaller, multiple in nature and periventricular in location with a predeliction for cerebellum(2). Treatment with intravenous methyl prednisolone (IVMP) followed by oral prednisone has been tried in cases of isolated optic neuritis(8) and for acute transverse myelitis. The additional benefits of this regimen were documented in patients with acute optic neuritis in the form of reduction in the rate of development of multiple sclerosis from 17% to 8% over a period of 2 years(9). The mechanism of action of methyl prednisolone is unknown, but it is shown to induce a transient lymphopenia with a significant reduction in CD-4 positive cells and interleukin-6 production by brain and spinal cord macrophages. Interleukin 6 regulates the production of antibodies and the cytotoxic activity of T cells. An accurate estimate of the survival and recovery rates in Devic's is difficult in part because of the variable pathological changes, disease associations and rarity of this disease. It is in general associated with a variable prognosis(1,2), though isolated cases have shown excellent recovery with steroids, as reported in the literature(10,11). In a series of 8 patients reported by Mandler et al. inspite of various immunosuppressive treatments, only one improved, 5 died and 2 patients were left with severe residual ambulatory and visual defictis(7). In a series of 9 Indian cases, with majority belonging to lower socio-economic group, Singhal and Wadia have reported partial remission in 4, the condition remained unchanged in 4 patients and one died(12). Our patient responded to high dose methyl prednisolone with substantial recovery of vision, motor and bladder function, within four weeks of treatment. Our patient remained symtom free 14 months into followup and is under close observation for clinical relapses as the possibility of Devic’s disease as a presenting manifestation of multiple sclerosis cannot be ruled out, even though CSF oligoclonal bands were negative and there were no characteristic periventricular lesions as seen in 90% of patients with multiple sclerosis. Contributors: RHM, SMJ and SM did the case work-up and drafted the paper. SMJ will act as guarantor for the paper. SJT and BE participated in data collection and reference work. Funding:
None.
|
![]()