|
Riyaz A.
Vinayan K.P.
From the Departments of Pediatrics Institute of
Maternal and Child Health, Medical College,
Calicut, Kerala, India.
Reprint requests: Dr. Riyaz A, Assistant Professor and Pediatric Gastroenterologist, Department of Pediatrics, Institute of Maternal and Child Health, Medical College,
Calicut 8, India.
Manuscript Received: December 17, 1997; Initial review completed: January 19, 1998; Revision Accepted: May 1, 1998.
Spinal cord compression is a rare complication of malignant tumors of childhood. The most common causes are bone and soft tissue sarcoma, lymphoma, leukemia and
neuroblastoma(1). They produce an acute block in the CSF pathway, owing to the rapid growth within the confined space. Such children usually present with flaccid paraplegia, urinary retention and patulous anus. Here we are reporting a rare case of intraspinal neuroblastoma,
which presented as acute flaccid paralysis, unfortunately following pulse polio immunization. A correct diagnosis was extremely vital in
this case, because of its serious consequences to the pulse polio proramme.
Case Report
A one-year-girl who was apparently healthy previously was admitted with a
history of insidious onset of weakness of both lower limbs, one week after a
pulse polio immunization. She had low grade intermittent fever for 3 days. There was no history of convulsions. She was conscious and oriented. The muscle power was Grade I in both lower limbs which became Grade a within 3 days of admission. The deep tendon reflexes were absent in the lower limbs and plantars were equivocal. Abdominal reflexes were normal. Sensory system and bladder functions could not be tested. The upper limbs and neck muscles were normal. She. did not have significant lymphadenopathy or hepatosplenomegaly. She was unimmunized, except for the single pulse polio vaccine.
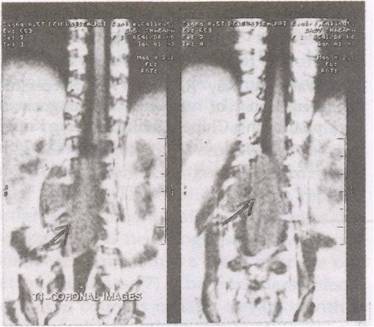
CSF showed features of Froin syndrome, the protein being 6g/dl. X-ray spine and USG abdomen were normal. MRI scan showed a large intradural lesion with extradural extension in L1 to L5 region, of intermediate signal density in both T1 and T2 weighted image (Figs. 1&2).
L3-L4 right sided laminectomy and
biopsy decompression were done under GA. Histopathology was suggestive of neuroblastoma. Twenty four hour urinary VMA level was normal. The neurologic
recovery was poor inspite of post-operative radiation.
 |
|
Fig. 1. T3 weighted
MR coronal images of the spine showing a large intradural tumor (arrow) with extradural extension
(L1-L5) with intermediate signal intensity. |
 |
|
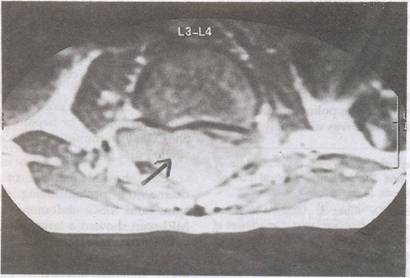
Fig. 2. T2 weighted
MR
axial
images of the spine showing the
tumor (arrow). |
Discussion
Spinal cord tumors are .rarer than intracranial tumors, in both adults and children. The ratio of intracranial/intraspinal neoplasms for children varies from 20:1 to 5:1(2). These are most commonly found In the thoracic spinal cord followed by cervical, thoraco-lumbar and lumbo sacral areas(3).
Signs and symptoms of spinal cord tumors are usually insidious and misleading. Because of the vague history and paucity of clinical signs initially, a definitive diagnosis may be delayed. The most common com- plaints are abnormalities of gait or pain in the extremities or back. In the very young, who are not bowel or bladder trained, sphincter abnormalities may be over- looked(4).
Traditionally, tumors of the spinal cord are divided into intramedullary and extramedullary. Extramedullary tumors usually represent benign neurofibroma or malignant metastases from tumors like
neuroblastoma. Neuroblastoma usually produces spinal cord compression, due to dumb bell extension of the tumor arising from the para-spinal sympathetic ganglia(5).
The point of interest in this case was the development of acute flaccid paralysis in an unimmunized child, following a dose of pulse polio immunization.
This created a lot of panic in the public and medical personnel and it would have been a severe set back to the entire Pulse Polio Immunization Programme, if the correct diagnosis had not been established in time.
|
1. Madero Lopez L, Marrino Arribas JM, Contra Homez, Martin Ramos N, Peres Juvado L. Spinal cord compression in
children with cancer. An Esp Pediatr 1990; 32: 423-426.
2.
Reimer R, Onofrio BM. Astrocytoma of the spinal cord in children and adoles- cents.
J
Neuro Surg 1985; 63: 669-675.
3.
Guidetti B, Mercuri S, Vagnozzi R. Long term results of surgical treatment of 129 intramedullary spinal cord gliomas.
J
Neurosurg 1981; 54:
323-330.
4.
Cohen ME, Duffner PK. Tumors of Brain and Spinal cord including leukemic infiltrates. In: Pediatric Neurology-Principles and Practice, 2nd edn. Ed. Swaiman KF St. Louis, Mosby Year Book Inc, 1994; pp 925-926.
5.
Cellis S, Calisti A,. Marino IR, Manzoin C, Pintos C, Ianelli A, et al. Dumb-bell neurogenic tumors in Children. Pediatr Med Chir 1990; 12: 41-44.
|
