TA 13-year-old boy was admitted with the complaints of gradual distension of the abdomen and dull periumbilical pain. Examination revealed distension of the abdomen with dullness. There was no organomegaly or
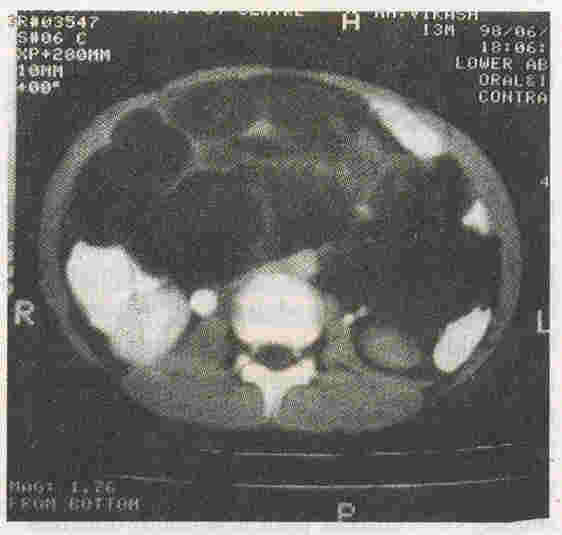
palpable lump. His blood investigations were normal. Ultrasound (US) abdomen showed a well-defined cystic mass with septae as well as some solid-honey-combed areas. CT scan abdomen revealed hypodense multicystic
cavities which did not enhance following intravenous contrast administration (Fig.
1).
Fig. 1. CT scan abdomen showing hypodense multicystic cavities which do not enhance following oral or intravenous contrast.
US-guided diagnostic aspiration revealed chylous aspirate. Laparotomy revealed a large cyst arising from the jejunal loop just next to the ligament of Treitz.
The cyst was occupying most of the mesentery and weighed 600 gram. The cyst was enucleated. Histopathology of the cyst revealed a lymphangioma.
The incidence of mesentric cyst is less
.
than one in 100,000 adult hospital admissions
and one in 35,000 pediatric admissions(1). The most common site is the small bowel messentery (70%) with 50-60% of all cysts located in the ileal mesentery(2). Ultrasonography abdomen reveals hypoechoic, uni-
or multi-loculated mass with septae(3). The treatment is complete enucleation of the cyst(2).
J.P. Soni,
B.D. Gupta,
M.P. Singh,
Meenakshi Soni,
Regional Institute of Maternal
and Child Health, Umaid Hospital,
Dr. S.N. Medical College,
Jodhpur, India.
1.
Kurtz RJ, Heimaun TM, Beck AJ, Mesenteric and retroperitoneal cyst. Ann Surg 1986; 203: 109-112.
2.
Chug MA, Brandt ML, Stuil D, Yazbeck S. Mesenteric cyst in children. J Pediatr Surg 1991; 26: 1306-1308.
3.
Hayden CK, Swischuk LE. Mesentery. In: Pediatric Ultrasonography, 2nd edn. Baltimore. Williams and Wilkins, 1992; pp 172-176.
|