|
Lymphangiectasia, characterized by dilated and proliferating lymphatic channels, is a benign lesion. Though regarded as malformation, the precise nature of this lesion whether hamartomatous or neoplastic
is uncertain(I,2). Overall the majority of these lesions are present in
childhood and the commonest sites are head, neck and axilla with fewer cases occurring in parenchymal organs(1,2). Involvement of intra-abdominal organs is quite rare, constituting 1.6% of all
cases(3,4). The most common, intra-abdominal location is the mesentry followed by omentum, mesocolon and retroperitoneum. Small intestinal involvement is extremely rare(5). A case of localized small intestinal lymphangiectasia is being reported for its rarity.
A four-year-old male child presented with pain abdomen, fever and vomiting for
one day. Abdominal examination revealed guarding and tenderness all over the
abdomen and bowel sounds were absent. Radiographic examination revealed multiple
fluid levels in the abdomen. Preoperative diagnosis of acute appendicitis was
considered. However, exploratory laparotomy revealed the presence of an oblong cyst measuring 12 X 13 cm on 'antemesentric border of ileum about 60 cm from ileocaecal junction. Resection of cyst alongwith ileal segment was done and end to end anastomosis performed. The post-operative period was uneventful.
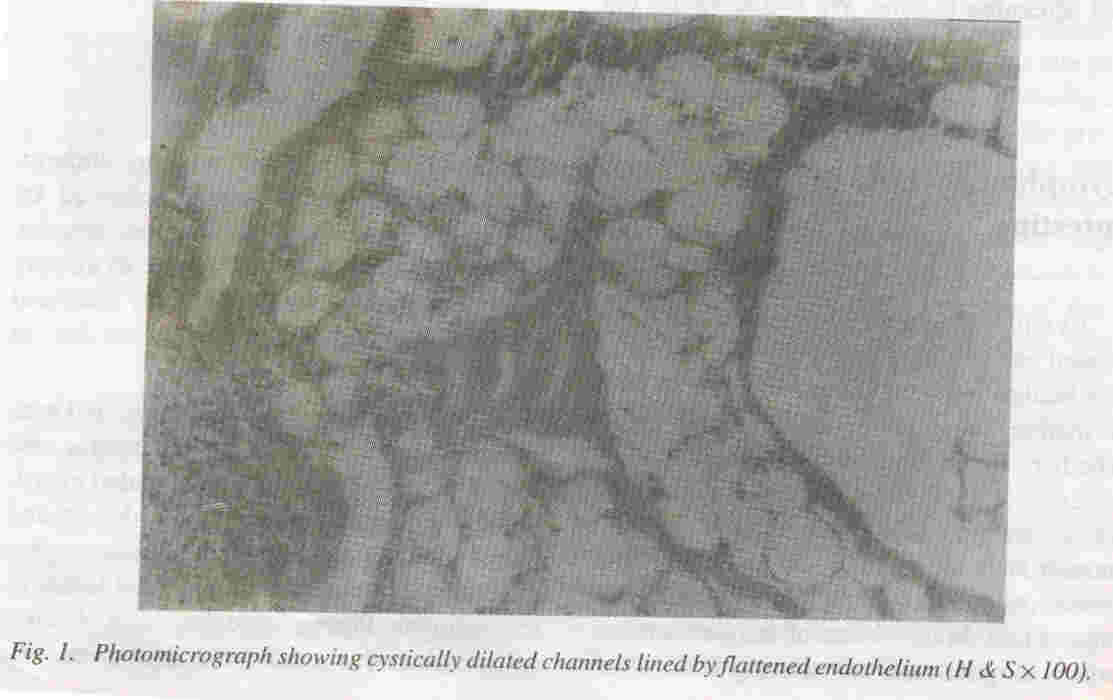
Gross examination showed a circum- scribed oblong cystic mass on the antemesentric border of small intestine. Cut surface showed multiple small cystic areas filled with white gelatinous material. Light microscopic examination revealed multiple cystic ally dilated anastomosing channels lined by a flattened endothelium (Fig. 1) ex- tending from submucosa to serosa of small intestine, intersecting and insinuating the layers of the wall of the intestine.
In this particular case, significant amount of capillaries and adipose tissue intermixed with lymphatic channels pointed to a hamartomatous nature. These lesions are benign and malignant transformation though reported is exceedingly rare(6).
Rajni Kaushik,
Shayam L. Kaushik*,
Jaishree Sharma,
B.B. Sharma,
Departments of Pathology
and Pediatrics; *
Indira Gandhi Medical College,
Shimla, Himachal Pradesh,
India.
|
1.
Ashley 018. Tumors vasoformative tissue. In: Evan's Histological Appearance of Tumors, 4th edn. London, Churchill Livingstone 1990; pp 77-108.
2.
Enzinger FM, Weiss SW. Tumors of lymph vessels. In: Soft Tissue Tumors. Eds. Enzinger FM, WeissSW. Toronto, TheC.V. Mosby Co., 1988; pp 614-637.
3.
Henzel U, Pories WJ, Brugerr DE, Smith JL. Intra-abdominal lymphangiomata. Arch Surg
] 966; 93: 304-408.
4.
Chaturvedi U, Singh N, Sakhuja P. Intra-abdominal Iymphangioma-Clinico-pathological profile of rare lesion. Indian J Pathol Microbiol 1977; 22: 563-566.
5.
Hamagiri T, Baba M, Shimabu Kuro,
Hashimoto M, Takemoto H, Inaue A, et a/. Lymphangioma in the small iitestine. Report of a case and review of Japanese Literature. Surg Today 1977; 22: 363-367.
6.
Bill AH, Summer OS. A unified concept of lymphangioma and cystic hygroma. Surg Gynec Obstet ]965; 120: 79-86.
|