|
Praveen Arora
Virendra Kumar
N.K. Dubey
K. Mahesh
From the Department of Pediatrics, Kalawati Saran Children's Hospital, Lady Hardinge Medical College, Bangla Sahib Marg, New Delhi 110001, India.
Reprint requests: Dr. Virendra Kumar, Associate Professor, Department of Pediatrics, Kalawati Saran Children's Hospital and Lady Hardinge Medical College, Bangia Sahib Marg, New Delhi-llOO01, India. Fax: 91-11-3363396
Manuscript received: September 18, 1998; Initial review completed: November 2, 1998; Revision accepted: December 14,1998.
Beta adrenoceptor blockers are commonly used drugs in clinical pediatric practice. Generally they are well tolerated, however accidental ingestion or poor elimination due to renal or hepatic functional impairment is known to increase their plasma levels which may result in serious toxicity such as bradyarrhythmias(1). The treatment recommended for such arrhythmia includes intravenous atropine, isoproterenol infusion, glucagon or cardiac pacing(2). We report a case of acute glomerulonephritis with atenolol induced bradycardia managed successfully with nebulised salbutamol.
Case Report
A ten-year-old boy, was admitted to the general pediatric ward for the treatment of
acute glomerulonephritis with left lower zone pneumonia. At the time of admission his heart rate was 86 per minute, respiratory rate 26 per minute, and blood pressure was 142/98 mmHg. Laboratory studies revealed hemoglobin 7.5g/dl, TLC-14100/mm3, blood urea 184 mg/dl, creatinine
3.8 mg/dl, serum sodium 131 meq/L, serum potassium 4.52 meq/L, ASO titer 400U/L, CRP 18 mg/ml, serum C3 levels 43 mg/dl. Urine analysis showed proteinuria (++), RBCs 60-80/HPF, epithelial cells and casts, X-ray chest revealed normal cardiac size and left lower zone consolidation.
The child received intravenous crystalline penicillin (2 lac units/kg/day) and gentamicin (5 mg/kg/day) in two divided doses; oral Atenolol2 mglkg/day, Furosemide 1 mg/kg/day and sublingual nifedipine 0.2 mg/kg/dose on SOS basis.
After one week of hospitalization the patient developed bradycardia (heart rate
40-47
beats/minute) and was transferred to Pediatric Intensive Care Unit (PICU) of Kalawati Saran Children Hospital, New Delhi.
On arrival to PICU, the child was conscious with heart rate of 45 beats/minute, respiratory rate of
18/minute and blood pressure of .104/72 mmHg. Jugular venous pressure was raised and liver was palpable 2.5 cm below the costal margin. No other cardiac abnormality was detected. Examination of the chest revealed left lower lobe consolidation and had no evidence of bronchospasm. Leg raising exercise in bed for two minutes did not increase the heart rate beyond 47 beats/ minute. Blood urea was-l13 mg/d1 , serum creatinine-1.8 mg/dl, serum sodium-138
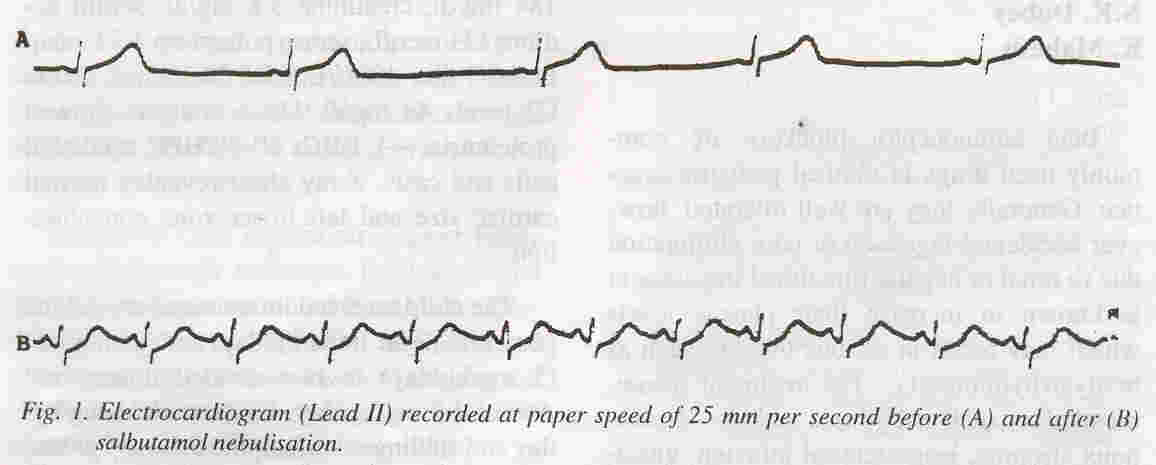
meq/L, serum potassium-4.46 meq/L and random blood sugar was 88 mg/dl. On chest X-ray cardiothoracic ratio was 56% and electrocardiogram was essentially normal except bradycardia (Fig. IA).
Atenolol was discontinued and the child was placed on a cardiac monitor (Hewlett Packard 78352). After six hours of observation the child was conscious and BP was
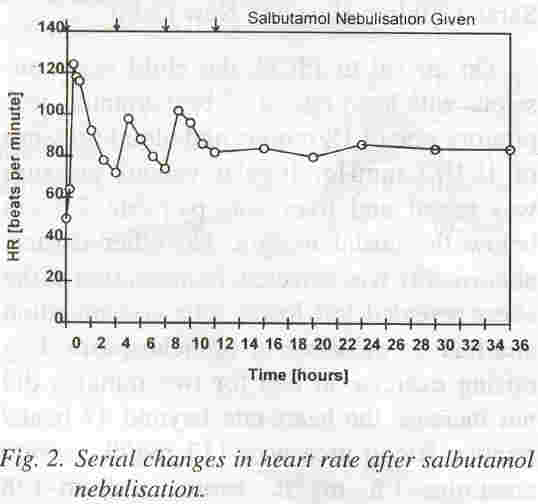
normal but due to persistent bradycardia and impending cardiac failure, a trial of nebulised salbutamol was planned. The child was given continuous salbutamol nebulisation (0.5 mg/ kg/hour) for 30 minutes. Heart rate started increasing after 15 minutes and reached a maxi- mum of 122 beats/minute after 30 minutes of nebulisation (Fig. 2). The ECG repeated after completion of nebulisation was essentially normal (Fig. J B), HR 100 beats/minute.
Subsequently, another three doses of nebulised salbutamol (0.15 mg/kg/dose) were given at 4 hour intervals. After stabilization of his heart rate to 80 beats/minute, no further nebulisation was given.
Discussion
To the best of our knowledge this is the first reported case of successful use of nebulised salbutamol to counteract the effect of atenolol. Serum atenolol
levels could not be assayed in this case; however, development of sustained bradycardia
in the child receiving a higher dose of atenolol in the setting of pre-existing renal impairment was highly suggestive of it being a atenolol related complication. A suboptimal increase in heart rate with exercise observed in our case has
also been shown to be a good indicator of
β
adrenoceptor blockage(2).
Atenolol is a competitive inhibitor of the effect of catecholamines at
β1 adrenoceptor sites without intrinsic activity. It is water soluble and excreted mainly by the kidneys. Slowing of resting heart rate is a normal response to the treatment with
β
blocking
drugs. Overdose however can cause severe bradycardia, heart block, hypotension,
cardiac failure and other metabolic and ventilatory insufficiencies( 1,3).
Conventionally intravenous atropine, isoproterenol or glucagon are used to treat bradyarrhythmia which need invasion. and maintenance of an intravenous line and close monitoring for potentially fatal dysarrhythmia and sudden death(2).
Though salbutamol is a selective
β2 stimulant with minimal cardiac
(β1) activity, tachycardia remains the commonest side effect(4). The same prompted us to try nebulised salbutamol in this patient. A significant increase in HR after 30 minutes of nebulisation in our case could be related to the presence of
β2
receptors in cardiac atria as demonstrated earlier(5) or to change in
number and sensitivity of the adrenoceptors to catecholamines. It has been observed that the
β
receptors are not static entities and are subject to a variety of influences regulating their sites and sensitivity to catecholamines. Prolonged exposure to
β -
blockers may increase the number of
β-receptors available for use at a given time and their withdrawal may result in an exacerbated response to
β-stimulants(6).
The positive response to nebulised salbutamol observed in our case however needs to be interpreted cautiously as the
manifestations and response to therapy for
β-blocker overdose is variable and influenced' by the age, the dose and duration of ingestion, pattern of metabolism and cardiovascular status of the patient(7).
Based on this single case observation it would be premature to suggest its use as definite first line therapy, but if it were to prove effective, it would be readily available and further research is suggested to define the efficacy and dosage of such treatment.
|
|
1.
Olin BR, Hebel SK. Drugs Facts and Comparisons. St. Louis, A. Wolters Kluwers Company, 1995; pp 801-815.
2.
Frishman WHo Overdoses with beta-adrenoceptor blocking drugs. 111: Clinical Phar- macology of the
β-Andrenoceptor Blocking Drugs, 2nd edn. Norwalk, Appelton-Century- Crofts, 1984; pp I 69-203.
3.
Hoffman BB, Lefkowitz RI. Beta-adrenergic antagonists. 111: Goodman and Gilman's The Pharmacological Basis of Therapeutics, 9th edn. Eds. Hardman JG, Limbird LF. New York, McGraw Hill, 1996; pp232-242.
4.
Spiller HA, Wiley JF, Krenzelok EP, Broys OJ. Accidental albuterol ingestion in children (Ab- stract). Vet Hum Toxicol1992; 34: 325.
5.
Motomura S, Zerkowske HR, Daul A, Brodde OE. On the physiologic role of ~2- adrenoceptors in the human heart: 111 vitro and ill vivo studies. Am Heart J 1990; 119: 608- 619.
6.
Frishman WH, Sonneblick EH. Beta adrenergic blocking drugs. 111: The Heart, Arteries and Veins, 8th edn. Eds. Schlant RC, Alexander RW. New York, McGraw Hill, 1994; pp 1271- 1272.
7.
Delima LGR, Kharasch ED, Butter S. Successful pharmacological treatment of massive Atenolol overdose: Sequential hemodynamics and plasma atenolol concentrations. Anesthesiology 1995; 204-207.
|