|
|
Case Reports Indian Pediatrics 2001; 38: 83-87 |
|||||||||||
|
Top-of-the-Basilar-Artery Stroke |
|||||||||||
|
Stroke is not an uncommon problem in children(1). In the last two decades anti-phospholipid antibodies (APLAs) have been recognized as an important cause of ischemic stroke. Of all ischemic strokes, middle cerebral artery distribution has been the commonest and posterior circulation the rarest(2). We report here a child with top-of-the-basilar-artery stroke due to APLAs.
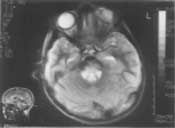
An eight-year-old boy presented with history of fever for 4 days and sudden onset blindness 12 hours prior to admission. There was no history of seizures, alteration of sensorium, headache or vomiting. There was no ocular pain or visual hallucinations. He was febrile at admission. All peripheral pulses were normal. He was normotensive. Other general physcial examination was unremarkable. Intermittently the patient lapsed into drowsi-ness. He had bilateral ptosis with complete blindness. There was up-gaze palsy with horizontal jerk nystagmus more on looking towards the left. Pupils were 3 mm in size and reacting normally. Fundus was normal. There was truncal and left sided limb ataxia. Rest of the neurological examination was normal. Other systems including cardiovascular were unremarkable. Analyzing the clinical findings further, bilateral ptosis, up-gaze palsy and drowsiness (involvement of the reticular activating system) point to a lesion in the high midbrain and/or thalamus. Cerebellar signs on both sides may implicate bilateral superior cerebellar arteries. Sudden loss of vision with preserved pupillary reflex suggested a bilateral posterior cerebral artery involvement. All of these features localize disease to the area supplied from the top of the basilar artery. On investigation, cranial MRI showed infarcts in both thalami (Fig. 1) and midbrain (Fig. 2). Investigations for a cause of stroke including hemogram, coagulogram, ANA, RF and LE cell phenomenon were all negative. There was no clue to infective endocarditis. Echocardiogram was normal. X-ray cranio-vertebral junction was normal. Anticardiolipin antibody (ACLA)-IgM level was 106.00 IU/ml by ELISA, a level above 65 IU/ml being considered as strongly positive. Transcranial Doppler study of vertebral artery did not reveal any abnormality. Lumbar puncture, initially withheld, was normal on day 10 of illness.
During hospital stay the child developed altered sensorium and abnormal posturing (decerebration on the left and decortication on the right). There was persistent left hemi-paresis and bilateral restriction of adduction of eyeballs. He was empirically started on anti-biotics for suspected pyomeningitis with vasculitis causing stroke. Decongestive measures (mannitol 0.25 g/kg/dose 4-6 hourly, frusemide 1 mg/kg/dose 12 hourly, optimum hydration, head propped up and minimal handling) were instituted and child was put on low dose aspirin. After 2 weeks he was discharged while on aspirin. After 3 months on follow-up he was ambulatory, spoke coherently although with mild dysarthria. There was return of some vision. There was minimal residual left hemiparesis and left III nerve palsy. Fundoscopy showed optic atrophy.
The incidence of ischemic stroke(IS) in children has ranged from 0.63 to 7.91 per lakh per year in various studies(3,4). Preceding fever has been reported in upto 55% of IS in children(1). Hence, presence of fever need not divert attention from stroke to infective space-occupying lesions in such patients. Children with major artery occlusion associated with bacterial meningitis have been reported(5). In our case although CSF reports were con-founded by prior antibiotics, we had a definite etiology of stroke as APLA. In children ischemic stroke has been most commonly reported in the distribution of the middle cerebral artery. Posterior cerebral and vertebrobasilar involvement have been dis-tinctly rare(2). In an Indian series of 43 children symptoms and angiographic demons-tration of vertebrobasilar artery stroke have been conspicuously absent(6). Hence, the rarity of the case described. Another feature in our patient was blindness without occipital infarcts. This was explained by involvement of the posterior visual pathway at the lateral geniculate body (LGB) or just proximal or distal to it. Optic atrophy detected on follow-up may, however, point to anterior ischemic optic neuropathy (secondary to APLA) as the cause of blind-ness. Also, posterior segment lesion in the visual pathway around LGB may produce optic atrophy as a manifestation of retrograde degeneration. Thalamic infarcts have been reported in 60 out of 377 adults in the New England Medical Centre Posterior Circulation Registry(7). In 13 cases the localization was at the top of the basilar artery which was the commonest finding. In a series of six children reported with ischemic infarcts(8), no patient presented with blindness. Altered consciousness, hemiparesis, ocular motility abnormalities were, however, seen in these patients as in ours. Bilateral thalamic infarction due to APLAs has been reported in a 16-year-old girl(9) who presented with hypersomnolence, impaired memory and mood disturbance. Comparing young adults and children, a prothrombotic state has been found to be more common in the latter group with ischemic stroke(10). The cause of a prothrombotic state in the index case was the presence of APLA. He did not fulfil the criteria for a diagnosis of antiphospholipid syndrome (APS) in the strict sense going by the suggested criteria(11). Thrombosis could not be demonstrated at the time MRA was done. Also, ACLA assay was not repeated as required by these criteria. Stroke is the most common manifestation of primary APS. Such strokes are often recurrent and accompanied by TIAs and retinal occlusive events(12). Children with stroke and APLA have been reported(13, 14). ACLA level was very high in the index case. In SLE patients with vessel occlusion it was seen earlier that ACLA level was the same in those with and without recurrent thrombosis(15). No sudden increase of ACLA level preceded thrombotic episodes. In these patients authors found IgM ACLA more reliable than IgG in predicting future risk(15). Prolonged anticoagulation is mandatory in such patients. Warfarin and aspirin have been tried. However, differences of opinion exist on the duration of therapy. Some workers recom-mend till APLA has been negative for 4-6 months while others suggest life-long therapy. We have reported here a child with top-of-the-basilar-artery stroke. Storke in this territory is almost always embolic in adults. Our case is unique as top-of-the-basilar-artery stroke was due to a prothrombotic state from APLA. Contributors: SM reviewed literature and drafted the case report. DG provided neurological expertise both in managing the case and formatting the report; he will act as the guarantor. RP was the resident taking care of the case and reviewed literature. VRP was responsible for overall supervision and also helped in drafting the paper. Funding:
None.
|
![]()