|
|
Case Reports Indian Pediatrics 2001; 38: 179-183 |
||||||||||
|
Post-transfusion Graft Versus Host Disease - An Under Recognized Entity |
||||||||||
|
Manuscript received: February 14, 2000; Human graft versus host disease (GVHD) has commonly occurred after allogenic bone marrow transplantation(1) and has occa-sionally been reported after solid organ transplantation(2). GVHD has also been reported to occur after blood transfusion and is now recognized to be rare complication of modern blood transfusion practice(3-6). Post transfusion GVHD (PT-GVHD) results in symptoms and signs each of which can be due to multitude of primary or treatment derived causes thus obscuring its clinical diagnosis. Additionally PT-GVHD is a delayed reaction and the illness is often not recognized to be with blood transfusion. PT-GVHD has a higher mortality than any other adverse effect of the transfusion and recogni-tion of the disease is frequently dependent upon clinical suspicion and interpretation of pathological findings by the pathologist(3-5). Proper recognition and documentation of the condition is necessary since the disease is believed to occur more frequently than is currently reported. The incidence of PT-GVHD in adults is reported as 0.1% to 1%(5) while no US figures on the incidence of PT-GVHD in exist. The data from Japan imply very high rates. Eleven per cent of the cases reported from the Japanese Red Cross PT-GVHD study group were in children less than 10 years old(6). Recently we came across two neonates with the clinical and histological features typical of this much under recognized condition. To the best of our knowledge there are no reports from India on PT-GVHD. In this paper, we have described their clinico-pathological features based on necropsy data in one and skin and bone marrow biopsy in other.
Two full term neonates weighing 2.4 kg and 3.7 kg developed neonatal hyperbilirubi-nemia due to ABO incompatibility and glucose-6-phosphate dehydrogenase enzyme deficiency, respectively. Double volume exchange transfusion was performed with 3 units and 1 unit of fresh whole blood, respectively. Both of them presented within one month of life with maculopapular rash all over the body which rapidly changed into blisters filled with clear fluid and then peeled off. Subsequently they developed fever. There was evidence of cellulitis of upper limbs in one of them and the other infant developed bronchopneumonia and conjunctivitis. Both of them showed progressive fall in blood counts with severe pancytopenia and absolute neutropenia. They also developed focal hypo-calcemic seizures with parathormone levels being elevated. CT scans of the heads were normal. One of them also developed conju-gated hyperbilirubinemia. In addition to anti-biotics and supportive treatment, both the infants had received GM-CSF in view of neutropenia but with only marginal increase in counts. A diagnosis of post-transfusion graft versus host disease was suspected. No immunosupressants were given to either of them. The first infant died at day 43 of life before any intervention and an autopsy was performed. The second infant underwent skin biopsy and bone marrow aspiration. He died at day 52 of life. Autopsy was refused by the parents.
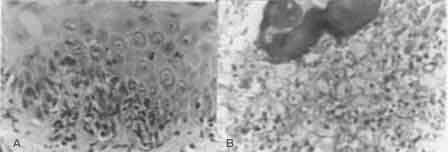
Case 1: There were mild scaly lesions on skin all over body. Skin biopsy showed hyper-keratosis, keratotic plugging in the epidermis, vacuolar degeneration of the basal layer with formation of dermoepidermal cleft. There was mild lymphocytic infiltrate in the dermis with foci of single degenerated, dyskeratotic keratinocyte surrounded by lymphocytes, a phenomenon known as "satellite cell necro-sis". The necrotic keratinocytes contained a pyknotic nucleus and eosinophilic cytoplasm (Fig. 1a). Liver showed moderate lymphocytic infiltrate in the portal tracts with preferential lymphocytic cuffing around bile ducts. Few bile ducts showed lymphocytic infiltrate in their wall. Thymus was atrophied and microscopi-cally it showed maintained folial architecture but the lobules appear collapsed and elon-gated, separated by fibrous tissue. Vessels were disproportionately large. There was loss of corticomedullary demarcation with marked depletion of lymphocytes and complete absence of Hassals’ corpuscles. An inflammatory infiltrate of plasma cells, neutrophils, and eosinophils was seen in the lobular and the interlobular septae. Inter-cellular hyaline like material was present along with hyaline thickening of the blood vessels. Immunohistochemically, lympho-cytes showed absence of both B and T cell markers. Spleen also showed atrophied white pulp with absence of T and B cell markers on lymphocytes. Lymph nodes were not enlarged grossly. Only an occasional lymph node in the anterior mediastinum was detected on microscopic examination which also showed lymphoid atrophy with loss of cortico-medullary demarcation. Bone marrow showed a distorted architec-ture and diffuse infiltrate by large histiocytic cells. The cells were large with pale, foamy cytoplasm and vesicular nucleus. Some of them showed erythrophagocytosis. There was almost a complete absence of normal hemopoietic elements (Fig.1b).
There was evidence of disseminated infection by Candida involving liver, spleen, both the kidneys, lung and thymus. Deep ulcers colonized by gram positive cocci were seen in whole of the gastrointestinal tract as well as an abscess in the spleen had gram positive cocci. All other organs including brain were normal. Case 2: Antemortem skin biopsy showed features similar to that of case one. Bone marrow aspirate revealed cellular fragment composed of large histiocytic cells with abundant pale cytoplasm and vesicular nucleus. Many showed evidence of erythro-phagocytosis. Normal hemopoietic elements were almost completely absent.
Graft versus host disease is a complication that follows infusion of histoincompatible lymphoid cells. PT-GVHD is often seen in individuals with severely impaired cellular immunity who cannot reject transfused leuco-cytes(3,5). In immunocompetent individuals, one way HLA match by transfusion of blood from a donor homozygous for one of the recipients HLA haplotype is believed to result in PT-GVHD(4). In this situation, the host cannot recognize foreign major histocompati-bility complex (MHC) antigens on donor cells and does not develop an immune response. PT-GVHD is also described in infants receiving in utero or exchange transfusion, extremely premature infants, neonatal allo-immune thrombocytopenia, and those under-gone extra corporeal membrane oxygenation. Antigens on the epithelial surface of skin, gut, liver and stem cells of bone marrow are major targets of GVHD. The disease manifests as fever, a maculopopular skin rash which may progress to generalized erythroderma and desquamation, diarrhea, hepatocellular damage with marked elevation of liver function tests and pancytopenia. The course of disease is rapid and carries a high mortality rate of almost 100%. These patients do not respond to immunosuppression or any other therapy currently in use(3-5). The characterstic histologic changes of PT-GVHD are seen in skin, liver, intestine and bone marrow. Skin biopsy, the least invasive and often diagnostic shows presence of ‘satellite cell necrosis’(7). Bone marrow reveals infiltration by histiocyte cells with erythrophagocytosis and aplasia of normal hemopoietic elements(8). In post mortem cases, thymic changes provide a clue to the immune status of the patient as in our first case. Using the criteria by Nezelof(9), thymic changes were of severe thymic atrophy secondary to graft versus host disease rather than the primarily dysplastic thymus. Use of fresh blood within 96 hours of collection is one of the most important risk factor predisposing to PT-GVHD as the viabi-lity of lymphocytes decline during storage(4). PT-GVHD has been reported with all kinds of cellular blood products including the stored one(5). It has been stated that 1×107 while cells per kg of recipients body weight are necessary to establish PT-GVHD(5). The use of white cell reduced blood components has been considered as a potential method of avoiding PT-GVHD. However, there are several reported cases of PT-GVHD in immuno-competent adults who received washed and filtered red cells(10). The latter component contains only 2 to 5 × 104 lymphocytes per kg of body weight which are far less than the stipulated one. Therefore, minimum dose of lymphocytes required to cause PT-GVHD is not known(5). Gamma irradiation of cellular blood products has been shown to reduce effectively the risk of PT-GVHD by inactivating the offending lymphocytes while maintaining RBC, platelet and neutrophil function(5). In conclusion, a high index of suspicion is critical to the diagnosis of PT-GVHD. The constellation of morbilliform rash, hepatic and gastrointestinal dysfunction and pancytopenia in a patient who has had a transfusion should alert the clinician to the possibility of GVHD. Skin and bone marrow aspiration/biopsy will suggest the diagnosis. Karyotyping (if the donor is of opposite sex), HIA typing of DNA analysis provides confirmation of diagnosis and may permit the identification of engrafted donor. GVHD is thought to be a preventable complication of blood transfusion. Irradiation of allogenic blood components to be trans-fused to susceptible recipients is recom-mended(5). Contributors: BJ worked up the whole case pathologically and drafted the paper. She will act as the guarantor for the paper. AN coordinated the study and helped in drafting the paper. RD participated in hematological work up and helped in drafting the paper.
Funding:
None.
|
![]()