|
|
Technology Update Indian Pediatrics 2001; 38: 147-156 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Mechanical Ventilation in Pediatric Practice |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Mechanical ventilation is the cornerstone of present day pediatric intensive care. In recent years, this modality has evolved into a highly specialized discipline(1). From the "iron lungs" used in the past primarily to treat respiratory paralysis in poliomyelitis, modern day ventilators have evolved into micro-processor based sophisticated devices capable of a large number of functions with many alarms to make them as safe as possible for the patient. This article attempts to briefly outline the salient features of mechanical ventilation in pediatric practice.
The term mechanical ventilation refers to various artificial means used to support ventilation and oxygenation(2). They encom-pass all forms of positive pressure ventilation as well as ventilators capable of taking over the entire function of breathing. In order to decide the need for mechanical ventilation, as well as monitor a patient it is worthwhile to familiarize oneself with some common terms and abbreviations shown in Tables I and II.
Mechanical ventilation is commonly deli-vered in intensive care by positive pressure ventilation. Positive pressure ventilation modes are defined by inspiratory events. Expiration is treated as an independent entity. The primary expiratory parameter, positive end expiratory pressure (PEEP) can be applied to any of the ventilator modes. Ventilator breaths may be classified based on three functions: initiation, limit and cycle off(2). These three phase variables determine events during inspiration (Table III).
The various modes of ventilation are classified based on the types of breaths that are selected. The modes most commonly used in pediatric practice are discussed here(3,4).
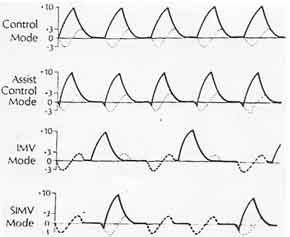
1. Controlled Mechanical Ventilation (CMV): In this mode, the ventilator controls all the ventilation while patient has minimal or no respiratory effort. This is the mode used at the initiation of mechanical ventilation. 2. Assisted Mechanical Ventilation (AMV): All breaths are triggered when the patient’s inspiratory effort exceeds the preset sensiti-vity threshold of negative pressure. In all other respects, it is similar to controlled mechanical ventilation. However, patients with central hyperventilation syndromes and tachypnea generate an extremely high minute ventilation. In contrast patients who are oversedated, or who are too weak to trigger the breath, may receive slow ventilator rates and inadequate minute ventilation. 3. Assist Control Ventilation (ACV): The problems with AMV described above have been addressed by the development of ACV, which is a combination of AMV and CMV. In this mode, the patient initiates the breathing as in AMV. However, if the patients fails to initiate the breathing within a prescribed time the ventilator triggers the breathing and provides a controlled breath as in CMV, thus ensuring a guaranteed minute ventilation. 4. Intermittent Mandatory Ventilation (IMV): It is essentially a combination of spontaneous breathing and CMV. A modified circuit provides a continuous gas flow that allows the patient to breathe spontaneously with minimal work of breathing, At a predetermined fre-quency, the ventilator provides a positive pressure breath to the patient. 5. Synchronized Intermittent Mandatory Ventilation (SIMV): In conventional inter-mittent mandatory ventilation, the controlled breaths may conflict with the patient’s own respiratory effort. SIMV overcomes this problem by allowing the patient to trigger the mandatory breath in the assist mode thereby synchronizing it with the patient’s respiratory effort. However, if the patient does not trigger a breath within an allotted time; the ventilator delivers a conventional breath.
1. Pressure Support Ventilation (PSV):In this mode, the patient triggers the breath as in assisted ventilation. Therefore, this mode is applicable only to spontaneously breathing patients. Once initiated the ventilator delivers air and gas mixture at a preset positive pressure in the ventilatory circuit. Patients determine their own inspiratory time and tidal volume. It is mainly used as a weaning mode and may be tolerated better than SIMV by some patients. 2. Pressure Control and Pressure Assist Control Ventilation (PCV and PACV): This is a time-initiated, pressure-limited and time-cycled mode intended for patients requiring total mechanical ventilatory support. Most ventilators also allow patient triggering of these breaths; producing pressure assisted breaths (pressure assist control ventilation).
PEEP is the most established means of providing airway pressure therapy. It can be added to every type of mechanical ventilation including spontaneous respiration where it is known as continuous positive airway pressure (CPAP). The primary goals of the use of PEEP are to increase the functional residual capacity, distend patient alveoli and recruit previously collapsed alveoli. This results in considerable improvement in gaseous exchange and improves SpO2 significantly. PEEP is generally started at a level of 3-5 cm water and increased gradually with the aim to achieve a SpO2 >90% with the lowest level of PEEP that allows FiO2 to be reduced to nontoxic levels (<0.5)(5). A very high PEEP (>15 cm water) can lead to air leaks, depressed cardiac output and barotrauma. The application of PEEP increases functional residual capacity and improves compliance of the respiratory system, result-ing in less work of breathing. PEEP is applied in case of most patients in pediatric critical care because of the unique characteristics of respiratory mechanics in children.
CPAP is best described as PEEP during spontaneous respiration. Infants with severe respiratory disease develop grunting which is a compensatory mechanism to elevate physiologic PEEP. In spontaneously breathing patients, CPAP can be administered through a valve or water column in the expiratory circuit. Most ventilators are, however, equip-ped with a CPAP mode. It can be administered through tight fitting mask, nasopharyngeal catheter, nasal prongs or through endotracheal tube. It is started at 5 cm water and increased by increments of 3 cm water while monitoring blood gases. If PaO2 remains <50 mm Hg despite CPAP of 10-12 cm water with FiO2 of 1, assisted ventilation is warranted. With improvement, CPAP is gradually reduced in steps by 2 cm water keeping a close watch on the condition of the patient and blood gases.
All modern ventilators are time cycled; in addition, these offer a volume controlled mode or a pressure controlled mode. Many present day ventilators provide both these modes. In general it is more convenient to utilize pressure preset ventilators with vari-able flow rates in infants under one year and volume limited ventilators in older children. However, any ventilator may be used pro-vided it has a sensitivity of volume adjust-ment adequate to make small changes that may be necessary in infants and young children.
Serious respiratory depression or paralysis causing hypoventilation or apnea is an obvious indication for mechanical ventilation. It should also be considered in patients who fail to achieve a PaO2 of 60 mm Hg at a FiO2 greater than 0.6 or those showing hypercarbia (PaCO2 >45-50 mm Hg). Mechanical ventila-tion may also be provided to lower PaCO2 levels in children with raised intracranial pressure.
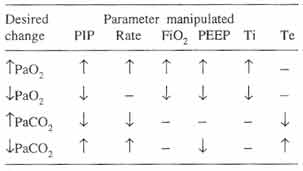
Before starting ventilation, it is standard practice to ensure that the ventilator must be clean and patient circuit sterilized. The humidifier should always be used. Ventilator parameters viz., rate, volume and/or pressure and appropriate alarms are set to desired level. The patients baseline data is recorded. After at least one minute of manually controlled ventilation with 100% oxygen by bag and mask, an orotracheal tube of appro-priate diameter is inserted by direct laryngo-scopy. If an artificial tracheal airway is needed for more than 12 hours, a nasotracheal tube is preferred. Adequacy of ventilation is assessed by the degree of excursion of chest wall, the presence of breath sounds bilaterally and the general response of the child. Ventilation should be started in the control mode with 100% oxygen to correct hypoxia and bring blood gas values towards normal. Once the child begins to breathe sponta-neously, ACV, IMV or SIMV modes may be used. The initial settings primarily depend on the nature of the lung disease as shown in Table IV and subsequently changes are made depending on the blood gases (Table V) and clinical assessment.
The initial settings in routine circum-stances are: FiO2 0.9-1 (may be lower in ventilation for neurologic conditions), PEEP 3-5 cm water, inspiratory time 0.75 seconds and respiratory rate of 20-25 per minute for children under 2 years and 15-20 per minute for older children(6). Tidal volume (10-15 ml/kg) should be adjusted to achieve visible chest excursion and audible air entry while maintaining a SpO2 >90% and PaO2 >60 mm Hg. FiO2 should be decreased to <0.5 as soon as possible to prevent oxygen toxicity and atelectasis. In chronically ventilated patients (more than 2-4 weeks), it is better to maintain the airway through a tracheostomy tube, since it is more comfortable, protects the airways and larynx and is less likely to be obstructed or inadvertently dislodged. Frequent suctioning, continuous humidification and meticulous wound toilet are necessary for care of the tracheostomy.
The initial evaluation and monitoring of a patient who needs assisted ventilation should include parameters such as respiratory rate, heart rate, blood pressure, core temperature and oxygen saturation along with degree of respiratory distress and neurological status. A chest X-ray film along with blood counts, electrolytes and cultures of blood, oropharyn-geal and tracheal suctions is obtained. While the child is on mechanical ventilation, the patients’ ECG, heart rate, blood pressure and blood gases are monitored. A record of FiO2, tidal volume, peak inspira-tory pressure, mean airway pressure and temperature of the inspired gases is main-tained. The inspired gas should be humidified to achieve a relative humidity of 80%(7). Regular physiotherapy and suction (maximum negative pressure limited to 50-100 mm Hg) is recommended. In addition to general supportive care, intake and output should be monitored closely and twice-daily weight record kept. The ventilator tubing is changed every 72-96 hours and the humidifier fluid changed daily. Sedatives and muscle relaxants are often needed to enable effective ventilation(8). These medications can be used on an inter-mittent dosing schedule or as a continuous infusion (Table VI). In most patients, sedation alone is sufficient. Muscle relaxants are needed in patients requiring maximal ventila-tory support and higher oxygen concentra-tions. It is important to understand that agitation frequently results from hypoxemia and correcting hypoxemia often obviates the need for further sedation.
A program for discontinuing mechanical ventilation (weaning) can usually be initiated when the following criteria are met(2):
During weaning, the emphasis is on ways of enhancing the return of full diaphragmatic function and discontinuation of mechanical ventilation(9,10). Weaning from pressure limited ventilators is usually achieved by gradual reduction of peak inspiratory pressure alternating with ventilator rate. After a peak inspiratory pressure of 20 cm of water has been reached, further reductions should be made only in the ventilator rate. Similarly, in volume limited ventilators tidal volume and rate are reduced step by step, and once a rate of 10-15 per minute has been reached, CPAP trials are initiated. The two most commonly used weaning modes are SIMV and PSV either alone or in combination(11). SIMV is generally success-ful in most patients. In this mode patient’s spontaneous breath rate and thereby his work of breathing is gradually increased by decreasing the mandatory ventilation rate. CPAP trials are used once the ventilatory rate is less than 15 per minute. Initially the patient is kept in a CPAP circuit for small-specified period on a regular basis e.g., five minutes 4 times a day, followed by full ventilatory support. The time period of CPAP is gradually increased until ventilatory support is discontinued. In PSV, once the patient has triggered the breath, a positive pressure in the circuit enables full tidal volume breathings. The method has the advantage of minimizing the work of breathing while making the patient initiate the breath. It also allows larger tidal volumes and better co-ordination with the ventilator. Children who have been ventilated for a period of less than 2-3 days and who were in good health prior to respiratory distress may usually be taken off straight from the ventilator and allowed to breathe sponta-neously. However, those patients who have been ventilated for a longer period need to be weaned gradually by allowing increasing periods of time for spontaneous ventilation over a period of several days. Throughout weaning, a close watch on the vitals must be kept and blood gases must be checked at the end of each weaning period off the ventilator. Respiratory depressants are to be avoided at all costs and additional humi-dified oxygen is given via tube during periods of weaning. Weaning may be difficult in certain patients (Table VII) and these factors must be addressed before initiating the process.
Mandatory minutes ventilation and mini-mal mandatory ventilation ensure delivery of a preset minute volume either by spontaneous breathing or assisted ventilation regardless of the respiratory drive. Inverse ratio ventila-tion(12) was specifically developed for patients with adult respiratory distress syn-drome. Inverse ratio ventilation with I : E ratio of 2-4 : 1 achieves better oxygenation by increase in airway pressure and progressive stabilization and recruitment of collapsed alveoli. High frequency ventila-tion provides very high respiratory rates of 5-25 Hz (300-1500 breaths per minutes) with very small tidal volumes(13,14). High frequency ventila-tion is primarily used as a rescue therapy for neonates failing on conventional ventilation. Liquid ventilation by instilling a perfluoro chemical in which both oxygen and carbon dioxide are highly soluble is an experi- mental method for achieving pulmonary gas exchange(15). Elimination of the gas liquid interface reduces surface tension resulting in increased pulmonary compliance and homogenous gas exchange.
As a complex and invasive technology, mechanical ventilation is fraught with numerous adverse outcomes, both iatrogenic and unavoidable. These need to be anticipated and managed promptly(16): 1. Airway Complications: Accidental tracheal extubation or obstruction of the tracheal airway by mucus or blood can be prevented by proper airway care, adequate humidifica-tion of the inspired gas, physiotherapy of the chest and frequent suction. Prolonged intuba-tion may lead to post-extubation subglottic bands, tracheal granuloma and fibrotic bands. Vocal cord damage and palatal grooves are also long term complications of prolonged mechanical ventilation. 2. Pulmonary Complications: Sudden hypo-xemia or deterioration in the circulatory status in a patient on mechanical ventilation warrants immediate examination to exclude tension pneumothorax. The danger of pneumothorax is increased and interstitial emphysema may occur when peak inspiratory pressure exceeds 40 cm water or when the end expiratory pressure exceeds 15 cm water. High pressure may also cause subtle and gradual changes such as leakage of fluid, proteins and blood into lung parenchyma. This is followed by an inflammatory response and reduced host defenses. Barotrauma can be minimized by maintaining low inspiratory pressure and tidal volume with minimum peak end expiratory pressure compatible with adequate ventilation. Prolonged exposure to high concentration of oxygen can damage the alveolar capillary membrane and produce congested edematous lungs with intra alveolar hemorrahge and exudates(17). Oxygen toxicity is suggested by increasing alveolar-arterial oxygen difference in the absence of pulmonary fluid accumula-tion. In neonates, a high oxygen concentration may lead to retinopathy of prematurity. Use of the lowest concentration of inspired oxygen to prevent hypoxemia is the best method to avoid pulmonary oxygen toxicity. General consensus indicates that FiO2 <0.5 can usually be tolerated satisfactorily. 3. Infection: Gram negative septicemia is the most common fatal complication in infants who require prolonged mechanical ventila-tion. The artificial airway and multiple intravascular catheters represent the route of contamination, and the hands of the professional personnel are the major vectors. Strict asepsis, daily change of the dressing and frequent changes of respiratory tubing are effective means to preventing infection. If infection develops, appropriate antibiotics should be administered, guided by culture/sensitivity patterns. 4. Other Complications: PEEP increases the intrathoracic pressure and reduces systemic venous return and cardiac output. These effects may cause serious consequences in patients with pre existing hypovolemia. They are overcome usually by increasing blood volume with or without inotropic agents(18). Thromboembolism from vascular catheters may lead to aortic thrombosis, renal impair-ment, cerebrovascular accidents and peri-pheral arterial occlusion.
The outcome of mechanical ventilation bears a direct relationship to the etiology of the primary physiologic impairment, available facilities and professional competence of the physicians and nursing staff. The survival rate of patients presenting with primary respiratory failure is high in experienced hands using standard equipment. In contrast, respiratory failure secondary to either circulatory or neurologic failure shows lower survival. Among survivors, nearly 1% develop chronic respiratory failure(2), which is defined as requiring mechanical ventilation for more than one month. Contributors: VNT drafted the manuscript and will act as guardian of the paper. SM did the research and also helped in drafting the paper.
Funding:
Nil.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()