|
|
Case Reports Indian Pediatrics 2000;37: 1380-1383 |
|||||||||||||
|
Basal
Artery Occlusion with Hyperlipoproteinemia Type IIb Causing Ischemic |
|||||||||||||
|
Ischemic stroke is an under reported but a significant cause of disability in childhood. In the United States the incidence of cere-brovascular disease in children is 2.5 cases per 100,000 population per year(1). When cerebrovascular disease occurs, the conse-quences are severe. In the majority of children who develop acute hemiplegia, no precise cause can be ascertained(2). The term acute infantile hemiplegia is applied to the sudden onset of pediatric stroke especially when no specific cause can be delineated(1). With advances in neuro-imaging, acute cerebral infarctions are becoming more readily visualized in children(3). Only a few cases of ischemic stroke in infancy have been reported in literature(4,6). We here report a case of ischemic stroke due to basal artery occlusion associated with hyperlipidemia, in a six month old infant.
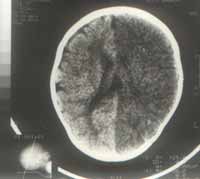
A six-month-old male infant was admitted to Sir Padampat Mother and Child Health Institute, Jaipur in December 1998 with com-plaints of repeated episodes of generalized seizures since last sixteen days and sudden onset of weakness in right upper and lower limbs two days prior to admission. There were no prior neurologic symptoms nor any history of fever, diarrhea, vomiting, ear discharge, trauma or bleeding from any site. The child was exclusively breastfed and develop-mentally normal. A history of sudden un-explained death was present in paternal grand uncle at the age of twenty years. Examination revealed that the child was obese with a weight of 9.1 kg (>90th percentile)(7) and triceps skin fold thickness of 15 mm (95th percentile). Body mass index was 19 (95th percentile). There were no tendon xanthomas. Blood pressure was normal and all central and peripheral pulses were of good volume and equally palpable. No bruit were heard over skull and carotids. Neurological examination revealed hypotonia with brisk deep tendon reflexes, ankle clonus and a power of 2/5 in right upper and lower limbs suggestive of upper motor neuron type right hemiparesis. Plantars were extensor bilaterally. Ipsilateral supranuclear facial weakness was also present. Neck rigidity and Kernig’s sign were absent and anterior fontanel was at level. Ocular fundi were normal. Liver span was 7 cm and spleen was not palpable. Other systems including cardio - vascular system were normal on clinical examination. The routine urine and blood studies including hemoglobin and platelet count, skull and chest roentgenograms, electrocardiogram and cerebrospinal fluid findings were normal. 2-D echo study of heart and Doppler study of extra cranial portion of carotids were also normal. The plasma was uniformly milky and formed no cream layer on top when stored overnight at 4°C. Fasting serum lipid profile revealed grossly elevated levels of total triglycerides and cholesterol, i.e., 664 mg/dl and 261 mg/dl (>95th percentile), respectively as compared to reported normal values of 195 mg/dl and 116-195 ± 37 mg/dl, respect-ively(8,11). HDL-cholesterol was 30 mg/dl, LDL-cholesterol was 98.1 mg/dl and VLDL was 132.8 mg/dl. The serum lipid profile of mother was in the normal range but breast milk fat content was 6.54% (as compared to normal mean values of 4.5%) which reduced to 5.7% on reducing dietary fat intake of mother. Other family members refused to undergo investigation. The electroencephalogram showed a diffuse left cerebral abnormality. CT scan head (Fig. 1) showed infarct in the territory of left middle and anterior cerebral artery. MRI angiography (Figs. 2 and 3) revealed bilateral stenosis of intra cavernous portion of internal carotid artery with relative thinning of left middle cerebral artery with paucity of distal branches with marked cortical atrophy on left side suggestive of basal artery occlusion without telengiectasia.
Hemiplegia secondary to vascular dis-orders occurs in children with an incidence of 3-8/100,000(12). Atherosclerosis has been incriminated as a rare cause of stroke in children(1). Changes in the intima with either multiple lipid laden plaques ulcerating into the lumen or an isolated atheromatous plaque may result in vascular occlusion(2). Accurate vascular localization is often possible in these cases by cerebral angiography/MRI angiography. Basal artery occlusion results from narrowing of the supra clinoid portion of the internal carotid artery or the proximal seg-ments of the anterior and middle cerebral artery(12). Lipoprotein abnormalities, parti-cularly those involving low levels of HDL and/or high levels of triglycerides or LDL levels, may mediate occlusive cerebro- vascular arteriosclerosis, and thus may pre-dispose children to ischemic cerebrovascular strokes(5). Increased levels of triglycerides and decreased level of HDL or both have been found in nearly 20% of unexplained stroke victims(12). Five patterns of elevation of hyper-lipoproteinemia type I to V have been identi-fied. Not all primary hyperlipoproteinemia manifests in childhood; primary type III has not been encountered in subjects under age twenty years and type IV and V only rarely so and that too in second decade of life(13). In contrast, primary type I and type II disorders are usually apparent in early childhood. Type I pattern consists of massive accumulation of chylomicrons in the plasma not attributable to recent fat ingestion, thereby forming cream layer on top of plasma when stored overnight at 4°C. Type II is characterized by increased concentration of LDL and total cholesterol without (Type IIA) or with (Type IIB) an increase in VLDL and triglycerides. When plasma triglyceride is over 600 mg/dl the plasma is usually opaque and ‘milky’ (lipemic, lactescent)(14). Age of presentation, elevated fasting total serum cholesterol and triglyceride levels, lipemic plasma with absence of formation of cream layer, BMI of 95th percentile favour hyperlipoproteinemia type IIb as the underlying liproprotein abnormality in this patient which could have been aggravated by consuming breastmilk rich in fat and thus contributing to cerebro-vascular compromise. Thus, in children with unexplained ischemic cerebrovascular accidents, the diag-nostic possibility of occlusive arteriosclerosis with thrombosis must be entertained(15). Many forms of lipoprotein abnormalities in children can be ameliorated by diet alone or by diet and drug therapy, approaches which can be used in affected children with stroke and their relatives. Contributors: All the authors contributed in the clinical workup of the case, discussion and interpretation of the findings, drafting of the article and final approval of the version to be published. SPC will act as the guarantor for the paper. Funding:
None.
|
![]()