|
|
Brief Reports Indian Pediatrics 2000;37: 1361-1367 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Preliminary Studies on IL-6 Levels in Healthy and Septic Indian Neonates |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sepsis is a major cause of morbidity and mortality during the neonatal period and its diagnosis still remains a major challenge to the pediatricians and neonatologists alike. The clinical symptoms are very often non-specific and subtle. As a result, in some cases, there could be a delay in diagnosis and manage-ment of infection, while in asymptomatic babies, there could even be over prescription of antibiotics. Several tests are available to detect neonatal sepsis. Total neutrophil count and the immature to total neutrophil ratio were earlier considered as excellent predictors of sepsis. However, studies conducted so far indicate that their levels get altered by several factors such as maternal hypertension, peri-natal asphyxia and intra-ventricular hemorr-hage(1). C-reactive protein (CRP) is another good marker for neonatal sepsis(2). It is known to be increased in both bacterial and fungal infections, but remains low in viral infection(2). However the CRP values do not rise significantly until almost 12-48 hours after the onset of infection. Blood cultures, the gold standard for the diagnosis of septicemia, requires up to 48-72 hours before the results are known and almost half of the positive samples do not show growth. Moreover, if the mother has received antibiotics before delivery, proper documentation of bacterial infection may not be possible. Various inflammatory cytokines such as IL-6, G-CSF and TNF alfa produced by monocytes and macrophages, and soluble receptors of IL-6 and TNF are known to be activated due to infection both in cord blood and in early neonatal period in healthy babies(3-11). IL-6 appears to be one of the promising candidate cytokine for diagnosis of neonatal septicemia(11). Cut off values for IL-6 levels in cord blood and early neonatal period have been shown to vary (ranging from 10-500 pg/ml) in different studies conducted in Western countries(5-7,10,11). This might reflect just different methods employed for estimations or some unknown factors. In the present study conducted in a metropolitan city, we assessed the levels of IL-6 in normal, healthy newborns of Indian mothers and also tried to evaluate the usefulness of IL-6 as a marker for sepsis detection.
Sample Collection from Normal Healthy Babies Cord blood (n = 49) and peripheral blood samples (24 hours after birth, n = 53) were collected from healthy babies born of single-ton vaginal deliveries without any perinatal complications. Forty of these samples i.e., both cord and peripheral blood were taken from a cohort of 40 babies whereas the remaining 9 cord blood samples and 13 peripheral blood samples were random of healthy babies. All these babies were dis-charged within a day or two after birth. Sample Collection from Septic Babies In forty babies (altogether a separate cohort of babies than the above normal cohort), blood samples were collected when they appeared clinically septic, within a week after birth. The clinical criteria taken as indicative of sepsis were:
Any feature from I and II associated with any symptom from III or any two features from I and II or from III would warrant a septic screen. This included blood collection for CRP, IL-6 and culture. Immediately after collection of blood sample, they were treated as neonatal sepsis (on clinical grounds). If after three days the patient was found to be normal (clinical and CRP), treatment was omitted and baby was discharged. Sample Collection from ‘High Risk’ Babies Blood samples were also collected from ten babies at risk for developing sepsis (features mentioned above in I and II) on days 1-3 even though no signs of sepsis were evident. Incidentally all these babies later developed sepsis and 8 of them were included in the ‘septic group’ of the study also. All the samples were collected irrespective of gestational age, birth weight, sex and day of life. Serum was separated, an aliquot was immediately frozen and stored at –70°C for IL-6 analysis while the remaining was used for CRP estimation. In babies with clinical suspicion of sepsis, blood samples were cultured to check for microbial growth. IL-6 Measurement Levels of IL-6 in the sera were estimated using commercial kits (Quantikine, USA) following manufacturer’s instructions. All the samples and standards were run in duplicate. Briefly, for sandwich ELISA, 100 ml of sample or standards were added per well in the 96 well plate pre-coated with monoclonal antibody directed to IL-6. After 2 hours of incubation at room temperature, the wells were washed four times with the wash buffer provided with the kit. Enzyme linked poly-clonal anti IL-6 antibody (200 ml) was then added per well and incubated for 2 hours at room temperature. After thorough washing. 200 ml of substrate (tetra-methyl benzidine) solution was added per well and incubated for 20 minutes in dark. The reaction was stopped by addition of 50 ml of 2N sulphuric acid to each well. The plate was read on ELISA reader at 450 nm and 540 nm, within 30 minutes. Wavelength correction, for correc-tion for optimal imperfection in the plate, was done by subtracting readings taken at 540 nm from readings at 450 nm. Standard curve was prepared from the serially diluted reagent provided by the manufacturer, against which the sample readings were plotted. The lowest detected value for IL-6 was 3.12 pg/ml and highest detectable limit was 300 pg/ml. The intra and interassay variation was less than 5%. CRP analysis and blood cultures were set up according to conventional methods.
(A) Healthy Babies CRP was undetectable in all the cord blood samples and in 49/53 peripheral samples collected 24 hours after birth. Details of the four healthy babies where CRP was found positive are given in Table I.
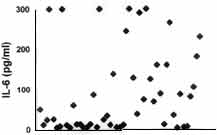
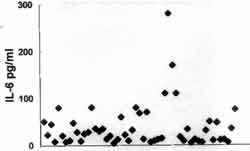
IL-6 levels (mean ± SE) were 90.9 ± 14.7 pg/ml in cord blood (n = 49) and 38.9 ± 6.5 pg/ml in peripheral blood samples collected 24 after birth (n = 53) with median values of 38 and 22.5 pg/ml, respectively (Table II). Mean values of IL-6 levels in cord and peripheral blood of 40 samples coming from the same 40 babies (whose cord blood was collected earlier) were 70 ± 13.8 and 42.14 ± 8.3 pg/ml with a median of 36 and 22.5 pg/ml, respectively. These were comparable to that of the randomly collected samples.
The scatter plots of the actual IL-6 values of healthy babies revealed a large variation in cord blood samples (Fig. 1a) which apparently stabilized in peripheral blood collected 24 hours after birth (Fig. 1b); with mean +2 SD value of 133 pg/ml. Since the values of IL-6 seem to have stabilized at 24 hours, our further studies were conducted only on samples collected 24 hours after birth and a cut off value of 133 pg/ml was considered as indicative of ‘high risk’ for sepsis.
Fig. 1. Scatter plots depicting absolute IL-6 values in normal babies in cord blood (Fig.1a) and 24 hours later in life (Fig.Ib) . All the values which fell out of range of our standards, were not further titrated to get absolute values, and have been taken as 300 pg/ml for plotting. (B) Babies With Clinical Suspicion of Sepsis Forty blood samples, collected on the day when sepsis became clinically evident (within a week after birth), were analyzed for CRP, IL-6 and microbial growth as depicted in Table III. As evident, CRP levels were found to be elevated in 21/40 babies whereas 16/40 samples exhibited growth in cultures. All the culture positive cases were also CRP positive. In five cases despite the presence of clinical signs of sepsis and elevated CRP levels cultures exhibited no growth. IL-6 levels were elevated (>133 pg/ml) in 18/21 CRP positive cases. Five out of thirteen babies where all three markers (CRP, IL-6, culture) were indicative of sepsis, expired. One baby with CRP and IL-6 positivity, one with IL-6 positivity, one with IL-6 positivity alone and one with neither IL-6 or CRP positivity also expired, may be due to extreme prematurity (28-30 weeks) with sepsis.
It has been suggested in earlier studies(10,13) that since IL-6 is required to induce CRP, IL-6 levels usually fall as CRP levels increase 12-48 hours after infection. This was evident in the present study also as only 8/12 CRP positive cases had ele- vated IL-6.
In order to study whether increase in IL-6 levels precedes the onset of infection, we further analyzed both CRP and IL-6 in blood samples collected from ten ‘high risk’ babies. The results indicate that CRP was negative in 9/10 samples collected at early time points (when there were no clinical evidence of sepsis) whereas IL-6 levels were more than 133 pg/ml in all the ten cases (Table IV). Moreover, in 2/3 cases where IL-6 levels remained elevated in serial samples, the babies expired. Prognosis of the babies was better in all cases where a fall in IL-6 levels was noted in the subsequent sample.
Evaluation of cytokines as early markers for sepsis has been well documented (3-11) and reviewed(12) in literature. Recently, Silveira and Procianoy(11) reported that IL-6 and TNF alfa are likely candidate cytokines for use in early diagnosis of neonatal septicemia. In the present study we have studied IL-6 levels in healthy newborn and evaluated its usefulness both when clinical signs of sepsis become evident as well as 3-4 days prior to clinical manifestation of sepsis. Preliminary results indicate that IL-6 could be used as an early marker for sepsis detection, 3-4 days prior to the clinical manifestation of sepsis. The normative data generated in the present study highlights the importance of time when sample should be collected for IL-6 measurement. As evident from Fig.1, cord blood may not be good sample to predict early onset sepsis in the newborn because 30% infants had values higher than 133 pg/ml. The IL-6 levels settle by 24 hours of life which appears to be an appropriate time for IL-6 evaluation. It has been reported earlier that no correlation exists between IL-6 levels in maternal blood and cord blood(7,10) indicating that IL-6 dose not easily cross the placenta and IL-6 in cord blood is perhaps of fetal origin. Moreover, their levels are known to be gestational age independent(6). Blood culture is the gold standard method to diagnose septicemia. In the present study, only 40% of cases with clinical suspicion of sepsis were found to be culture positive, with Klebsiella pneumonie being the most common pathogen. In nineteen babies, where IL-6 and CRP were measured when clinical signs of sepsis became apparent, the results showed that IL-6 does not appear to be any more useful than the usual CRP test since in 12 cases which were CRP positive only 9 had elevated IL-6 levels (Table II). It has been earlier reported that IL-6 levels usually fall as CRP levels increase 12-48 hours after infection(10,13, 14). Buck et al.(5) observed that IL-6 decreased within 24 hours to undetectable levels in majority of their infected infants. This could be due to the short half life of IL-6 as it can bind to plasma proteins such as alfa 2 macroglobulin, it shows early storage in the liver or its synthesis can be inhibited by other cytokines. This leads to an increasing proportion of false negative findings when sampling is performed later in the course of disease and probably explains the reduction in sensitivity with increasing postnatal age(10,14). In the preliminary analysis conducted on ten blood samples, collected prior to the appearance of clinical signs of sepsis, it was evident that IL-6 alone (CRP was negative in 9/10 cases) was indicative of onset of sepsis in all the ten cases at least 2-4 days prior to appearance of clinical symptoms (Table II). Persistent elevated IL-6 levels, in the present study, were found to be associated with bad prognosis as indicated by death or long term hospital stay. Since 9/10 of these cases were born preterm, it is evident from our pre-liminary results that IL-6 measurement (24 hours after birth) in preterm babies may prove to be beneficial in their management in the NICU. A pre-term baby with elevated IL-6 may be treated 2-4 days earlier even before the appearance of clinical signs of sepsis. On the other hand unnecessary administration of antibiotics and NICU stay could be avoided in pre-term babies with low IL-6 values. Similar observations have been made recently(15).
We wish to thank Dr. Sudha G. Gangal, Director, Research Society for her advice and help. The authors also thank Deepak Modi, Dilip Bagal, late Dr. Urvashi and the whole team of doctors at NICU, NWMH who helped in the study. Contributors: DB co-ordinated the study design, interpretation and drafted the manuscript. She will act as the guarantor of the paper. CK helped in sample collection, performing the test, data compila-tion and drafting of the manuscript. KS was the clinical collaborator, participated in both study designing and interpretation. HS was a clinical collaborator, participated in study designing, inter-pretation and manuscript preparation. RK was responsible for microbiology culture, RHM was clinical collaborator, arranged finances, participated in study designing, interpretation and manuscript preparation. Funding:
Mr. Ashwin Dand.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()