|
|
Original Articles Indian Pediatrics 2000;37: 1307-1313 |
|||||||||||||||||||||||||||||||||
|
Transcatheter Closure of Patent Ductus Arteriosus |
|||||||||||||||||||||||||||||||||
|
Key words: Amplatzer duct occluder, Gianturco coils, Patent ductus arteriosus. SURGICAL ligation and division of patent ductus arteriosus (PDA) has been a standard for treatment of patients with patent arterial ducts(1,2). With recent advances, catheter occlusion has become most attractive method for treating a persistent ductus arteriosus. The percutaneous technique was first described by Porstmann et al.(3). Since then various devices such as Rashkind double – umbrella occlusion system, buttoned device, Botalloccluder, PDA coils and more recently the Amplatzer duct Occluder have been introduced(4-8). In this study we present our results with the use of spring coils and the Amplatzer device.
This retrospective study was divided into two phases. Phase 1 : This was between October 1996 to July 1998. Patients with PDA less than 6 mm in diameter underwent attempt at coil closure of the duct and those with arterial duct bigger than 6 mm were referred for surgery because of high risk of coil embolization. Phase 2 : This was between August 1998 to December 1999, when no patients were directly referred for surgery, unless patients themselves opted for it. All patients who were diagnosed as having isolated patency of the arterial duct on echocardiographic evaluation were considered as potential candidates for non-surgical closure. Patients were advised to undergo coil occlusion of PDA if the estimated diameter of the PDA was less than 2.5 mm, and a device was preferred if the measured size of PDA was larger than this. An informed consent was obtained from the patients/parents for nonsurgical closure of the arterial duct. Spring Coils : Stainless steel coils 0.38mm diameter were used to close the PDAs (Fig. 1). The procedure has been described by Moore et al.(9).
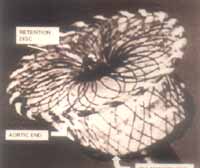
The Amplatzer Duct Occluder (Fig. 2) has recently been introduced as an alternative to surgery or other devices as a means of closing moderate to large sized PDA’s. It is a self expanding mushroom shaped device made from Nitinol wire mesh. The PDA is closed by induction of thrombogenesis, which is accomplished by the polyster fiber sewn securely into the device. The devices are cone shaped and 7 mm in length, with recessed screw, sizes are given from larger to smaller diameter. The delivery system consists of a delivery cable, a long sheath, loader and pin vise. The procedure followed has been described by Marwah et al.(8).
Residual Shunts The presence or absence of "immediate" residual shunting following coil or device implantation was determined by cineangiography, 10 minutes after the implantation. Residual shunt was classified as trivial shunt if there was only foaming seen but no jet across the device, mild shunt if there was a jet seen to be filling the left pulmonary artery but not the main pulmonary artery. Additional coils were deployed if there was residual shunting after coil deployment. However, no further attempts were made to achieve complete closure in the immediate period after device deployment. After 24 h of coil or device closure of the arterial duct, chest radiographs in posteroanterior and lateral positions were obtained to assess the coil or device position as the case may be. Complete echocardio-graphy and Doppler study was performed on all patients looking for residual shunt and left pulmonary blood flow obstruction. The ductus was considered fully occluded if no residual shunting was seen by color-flow Doppler. Follow-up All patients were followed-up on OPD basis and underwent complete echocardio-graphic and Doppler evaluation at 3 mo, 6 mo and 1 yr of the procedure. We carefully looked for residual shunts and any evidence of left pulmonary artery (LPA) stenosis on each visit.
A total of 121 patients were screened for patent ductus arteriosus. Forty eight of these patients underwent coil closure of PDA and 44 patients had device closure of PDA. Twenty nine cases were referred for surgical closure. Details of these patients is given in Table 1.
Coil Closure Group Forty eight patients underwent attempted coil closure of the patent arterial duct at ages ranging from 4 mo-480 mo (mean 78 mo). The procedure was successful in 42/48 (87.5%) patients. The duct size ranged between 1.6 mm-6 mm (mean 2.8 mm). A total of 48 procedures were carried out. Five patients underwent repeat coil placement between 3 mo to 6 mo of the first procedure , for residual shunts and one patient required placement of Amplatzer device and coil removal for the ongoing hemolysis. Twenty one of forty two (50%) patients had immediate complete closure of PDA, as seen on 10 minutes post-deployment angio-gram. After 24 hours of the coil deployment, 27/42 (64%) patients had no residual shunt on echocardiographic evaluation. Residual shunt-ing was seen in 9/42 (21%) patients at 3 months, in 4/42 (10%) at 6 months and only 2/42 (4.7%) at 1 year. These patients have not been seen at completion of 1 year, thus achieving a cumulative closure rate of 96% at the end of one year. Device Closure Group Forty four patients underwent device closure of PDA at ages ranging from 6 mo to 360 mo (mean 83 months). The duct diameter ranged between 2.8 mm to 10 mm (mean 4.4 mm). The device was successfully deployed in 42/44 patients. The device ranged between 6/4 mm to 14/10 mm. Complete closure of PDA was achieved in 23/42 (55%) at 10 minutes as seen in post-deployment angiogram. Trivial residual shunt was seen in 12/42 (28%) and mild residual shunt in 9/42 (17%) patients. Trival residual shunting persisted in 5/42 (11%) patients and mild shunting in 1/42 (2.7%) patient at the end of 24 hours. Of the 5 patients with trivial residual shunt at the end of 24 hours, 3 patients have been seen at 3 months; evaluation with 2-D echo and colour Doppler interrogation revealed complete closure of the arterial ducts. Two patients with trivial and one patient with mild residual shunts at 24 hours are yet to be seen at 3 months and 8 have completed 6 months of follow-up with repeat echocardiography and Doppler, all had device securely in place. There was no residual flow. Unsuccessful Attempts We were unsuccessful in eight of our attempts. There were 6 failures in the coil closure group and 2 in the device closure group. The unsuccessful attempts in the coil closure group were due to coil embolization while attempting closure. In the device closure group, one patient was a 4-month-old boy with PDA measuring 3.9 mm. A 6/8 mm device prolapsed through the ductus; the next available size (8-10-mm) caused obstruction to the descending aorta. The other patient was a malnourished 1 year old girl, weighing 4.8 kg, with PDA measuring 6.7 mm on angiography. Her PDA was considered to be too big for the device, considering her age and low weight. All these patients have been operated successfully. Complications Coil embolization was seen in 11/48 (23%) patients of the coil closure group. The duct diameter in these patients ranged from 2.4 mm to 6 mm (mean 4.3 mm). Six of these patients were subsequently referred for surgery whereas we were able to achieve closure of the patent arterial duct in the other five patient with coils only. The embolozied coils could be retrieved in all but one patient using a snare. Left pulmonary artery (LPA) stenosis occurred in 4/42 (9.5%) patients in the coil closure group and none in the PDA device group. The stenosis was mild in 3 patients and did not need any intervention, one patient developed severe stenosis of the left pulmonary artery and has been advised surgery. Hemolysis occurred in one of our patients following coil placement. The duct diameter in this patient measured 2.9 mm and 5 ´ 5 mm coil was placed in the duct as primary procedure. He developed severe hemolysis after 24 hours of the procedure. Second procedure was planned on the third day. Previously deployed coil was removed and Amplatzer device 6/8 mm was successfully deployed, resulting in complete closure of the arterial duct and this stopped the ongoing hemolysis. He developed mild jaundice and also required blood transfusion. Loss of distal pulse in right leg was seen in one patient after the procedure. This patient was put on heparin transfusion for 48 hours, following which the pulse became palpable in the right leg. The right leg pulse continued to be feeble as compared to left leg even at the time of discharge.
Excluding preterm newborns, the incidence of PDA is 0.05% accounting for 5 to 10% of all congenital heart disease. Most ducts are small to moderate and are hemo-dynamically well tolerated, but they carry a risk of bacterial endocarditis as high as 0.45%. Therefore it is accepted that all audible PDAs should be closed. The degree of hemodynamic compromise and possibility of spontaneous closure influence timing of closure during the first 6 months of life(10). Spring coils have been used throughout the world for PDAs up to 2.5-3 mm. Several studies using standard procedure, including a total of 425 patients have documented minimal complications and excellent cumulative occlu-sion rates. Complete occlusion was seen in 59-93% after 10 minutes, in 80-93% after 2-24 hours and 94-100% after 3-6 months. Inadvertent embolization occurred in 1-6% patients(11-14). Embolizations have been up to 16% in ducts measuring 4 mm or more(15). Our occlusion results, using coils are similar to those reported world-wide, 90-92% patients achieved complete closure by 6 months. However, in our study coil embolization rate was higher namely 22%. This was partly associated with our use of more than one coil especially for large ducts to achieve closure. Stenosis of the left pulmonary is a known complication following closure of the patent arterial ducts using coils. Various authors have reported the incidence between 10% and 18%(15,16). In our study LPA stenosis occurred in 4 patients; however, it was severe in only one patient. This patient had a duct measuring 4.5 mm and required 3 coils for complete closure of the arterial duct (8 mm, 10 mm and 5 mm). He has been advised to undergo surgical treatment. We have however not seen recanalization of previously occluded duct in our series as has been reported by Ino et al.(17). For the device closure group, complete closure was seen in all the 34 patients at the end of 3 months. Our results are in close comparison to those reported by Masura et al.(18). There was no incidence of LPA stenosis or device embolization in this set of patients. Ever since we have started using Amplatzer device for ducts larger than 2.5 mm, our success rates have increased and there has also been marked reduction in complications related to coil closure of bigger ducts. However, the current device is still not suitable for use in very small infants with relatively larger ducts. This is clearly evident by the two examples in our own study. Along with high cost, limited follow-up data, this may be a limitation of the current design of this device. In conclusion, in our experience most PDAs can be successfully closed with currently available spring coils or the Amplatzer device. Small residual shunts are common after the initial procedure, most tend to close off spontaneously. Some patients especially smaller infants with large ducts may still continue to require surgical closure of PDA until the limitations of the device size are removed. Contributors : SS co-ordinated the study (particularly its design and interpretation); she will act as the guarantor for the paper. AM participated in the interventional procedure and was responsible for data collection and drafting the paper. SR participated in all interventions and helped in drafting and critical analysis of the study.
Competing interests:
None stated.
| |||||||||||||||||||||||||||||||||
![]()