|
|
Letter to the editor Indian Pediatrics 2001; 38: 431-432 |
|
|
Hepato-Cerebral Complications in Ascariasis |
|
|
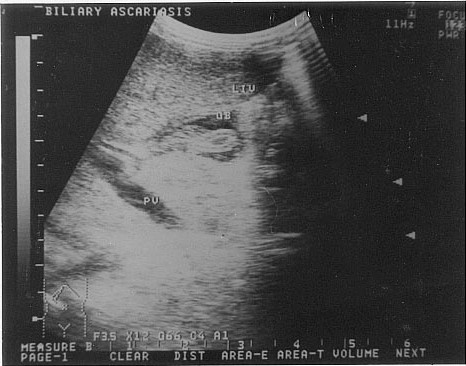
A 4-year-old male child, with a history of passing a worm ball in stools and 1 round worm through his vomit was brought in deep coma. On admission, his Glasgow Coma Scale (GCS) was 4. The peripheral blood count was 16000/cu mm and eosinophil count was 800/cu mm. Cerebrospinal fluid examination and serum electrolytes were normal. The child was given intravenous fluids and dexamethasone 0.3 mg/kg/dose 8 hourly. Within 24 hours, his GCS became 7 and in 36 hours he showed dramatic improvement with a GCS of 11. The cranial nerves, motor system, reflexes and fundus examination were normal. On the 2nd day of admission, the child developed an icteric tinge with prutitis, which progressively increased by the 3rd day. His liver function tests were: total bilirubin 9.0 mg/dl (direct 6 mg/dl), SGPT-580 IU/L, serum alkaline phosphatase 620 IU/L. Neuro-logically the child was totally normal with no focal deficits. An ultrasonography of the abdomen was done which revealed a roundworm in the gallbladder (Fig. 1) giving rise to obstructive jaundice. Serum IgE was raised to 430 IU/ml. A dose of antihelminthic (Mebendazole 100 mg/kg twice daily for three days) was given. The biliary ascariasis was surgically treated and the child recovered with no neurological or hepatic sequalae. Extraintestinal complications of ascariasis involve the pulmonary, hepato-biliary, and the central nervous system. Ascariasis is also known to mediate an immunological response. The clinical features of ascariasis relate to both larval and adult stages and depend on the intensity of infection. Migration of larvae through the lungs, particularly in heavy infestation, may cause a severe immune-mediated inflammatory response resulting in pneumonitis, liver enlargement and general-ized toxicity(1). The important hepatobiliary complications include acute cholecystitis, acute cholangitis, biliary colic, acute pancreatitis, hepatic abscesses, pyogenic cholangitis, intrahepatic duct and bile duct calculi due to dead worms forming the nidus of stones(2). Toxic cerebral symptoms simulating encephalopathy or meningitis have been reported earlier. The nervous symptomatology so often associated with ascariasis has been attributed to either the adverse effects of toxins produced by the larval or adult worms or their metabolities like acetaldehyde(3). Another hypothesis extended is an allergic or immune mechanism involving an antigen-antibody type of reaction in hypersensitive nervous tissue(3). However, the exact mechanism still remains far from clear. In conclusion, ascariasis should be considered as a differential diagnosis for a variety of obstructive hepato-biliary patho-logies and unexplained encephalopathy in a tropical country.
Sonali S. Bapat,
|
![]()