|
|
Case Reports Indian Pediatrics 2001; 38: 419-422 |
|||||
|
Castlemans’s Disease : An Unusual Presentation in Cervical Region |
|||||
|
Castleman’s disease is an unusual lymphoproliferative disorder of unknown cause. It is a clinicopathological diagnosis. We report the hyaline vascular variant of this entity occurring in the cervical region of a child. Reactive lymphoproliferative process in response to an unknown stimulus and defective immunoregulation may be involved in its pathogenesis(1).
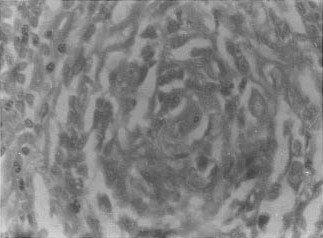
A 12-year-old boy presented to the Surgical Out Patient Department with a lump in right cervical region since 3 months. On further inquiry he gave history of constitutional symptoms like low grade fever since 2 months and loss of appetite. General examination was unremarkable and local examination of the region revealed a 7 cm ´ 4 cm nontender lymphnode mass with irregular surface and a firm consistency. His hemoglobin was 11 g/dl, total leukocyte count was 7600/cu mm (P: 45, L: 40) and ESR was 37 mm at the end of one hour. X-ray chest was normal. Fine needle aspiration cytology was reported as reactive hyperplasia. In view of strong clinical suspicion of tuberculosis, lymph node biopsy was performed. Histopathological examination revealed concentrically layered (onion-skin like) follicular cells with squamatoid appear-ance and a pseudofollicle with a hyalinized vessel suggestive of a variant of Castleman’s disease (Fig. 1). In view of this report we excised the whole mass. Six months after surgery, the patient was asymptomatic and there was no local recurrence. The patient was advised to follow up periodically at an interval of 3 months.
Castleman’s disease is a benign lympho-proliferative disorder characterized by enlarged hyperplastic lymph nodes which is rare in children(2). In 1956 Benjamin Castleman and his associates described this disease(3). Since then it is also recognized as angiofollicular lymphoid hyperplasia, giant lymph node hyperplasia, lymphoid hyperplasia, benign lymphoma, and follicular lympho-reticuloma(4). It can present as a localized mass or as a multicentric disorder. Its presentation as primary cervical lymph-adenopathy accounts for only 6% of cases reported in literature(5). Histologically, three variants are recognized, viz., hyaline vascular, plasma cell type, and intermediate type(6). Hyaline-vascular type is the most commonest presentation. This type is usually localized to mediastinum or pulmonary hilum(7). This is in contrast to our patient who presented with cervical lymphadenopathy. Parez et al. reviewed 76 cases of Castlemans disease reported in literature in pediatric age group and found that 54% of them had a localized hyaline vascular type of disease in mediastinum and rarely in cervical region as compared to the plasma cell type which occurred in 24% of the patients(8). It has been recently suggested that an abnormal production of a B cell growth factor, such as IL-6, causing lympho-proliferation and plasma cell differentiation may be the key factor in pathogenesis of Castleman’s disease(7). Localized disease usually has a benign course and can present as an asymptomatic mass or with compression effect in respective area and also as pyrexia of unknown origin, weight loss or anemia(9). Multicentric disease is a usually a systemic illness involving retroperitoneum, neck, parotids and muscles or it can present as a disseminated lymphadenopathy. It is aggressive and usually the fatal course is associated with infectious complications and risk for malignant tumors such as lymphoma or Kaposi sarcoma. The classical histopathological picture consists of presence of thickened hyalinized capillaries within the follicle centres. Also there is perifollicular vascular proliferation with concentric layering of cells within germinal centres. There may be more than one germinal center within a single follicle. Following the histological report, we excised the whole mass as surgery is curative for localized disease. Multicentric disease is usually associated with systemic manifestations and its prognosis is guarded. Its management includes a multimodality approach comprising of surgery, combination chemotherapy, steroids and radiation. lately anti-interleukin–6 receptor antibody therapy has been tried(10). Contributors: RSR was responsible for reviewing the literature and drafting the paper; he will act as guarantor for the paper. RA and KCV helped in drafting the paper.
Funding:
None.
|
![]()