|
|
Case Reports Indian Pediatrics 2001; 38: 411-414 |
|||||
|
Acquired Lobar Emphysema – An Unusual Cause of Respiratory Distress |
|||||
|
Lobar emphysema is one of the life threatening respiratory surgical emergencies. It can be either congenital or acquired(1). Acquired lobar emphysema usually occurs in the presence of a risk factor(2). We are reporting an unusual case of lobar emphysema in a neonate.
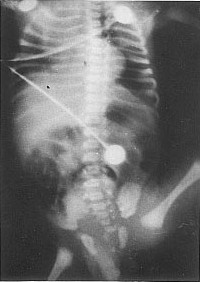
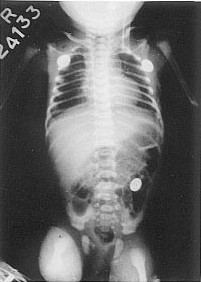
A primigravida mother gave birth to a term, male baby by elective Caesarean section for oligohydramnios. The birth weight of the child was 2.2 kg. Apgar score was 8/10 and 9/10 at 1' and 5', respectively. The baby was apparently normal and on breast feeds till 20 hours of life when he developed acute onset of respiratory distress associated with fever. The baby had an axillary temperature of 100.5° F with a respiratory rate of 80/minute. He had mild grunting with subcostal indrawing. There was good air entry on either side without any adventitious sounds. Examination of the other systems revealed no abnormality. A clinical diagnosis of neonatal septicemia with bronchopneumonia was made. Hemoglobin was 13 g/dl; total leukocyte count 18000/cumm with neutrophils 20%, lymphocytes 78% and eosinophils 2%. MicroESR was 4 mm/h and band cell count was 12%. Blood sugar and serum electrolytes were normal. A chest skiagram taken at this time showed haziness of the left upper and middle zone and air bronchogram suggestive of pneumonia (Fig. 1). The child was started on intravenous fluids, oxygen by hood and antibiotics (cefotaxime and amikacin). The child was stable initially, but suddenly deteriorated 12 hours later and developed central cyanosis. Pulse oximetry showed an oxygen saturation of 80% and arterial blood gas revealed type I respiratory failure (pH - 7.35, pO2 - 57.9, pCO2 - 29.9, HCO3 - 16.6 meq/L, O2 saturation - 86.6%, AaDO2 - 198.2). There was no evidence of pneumothorax. He was given endotracheal CPAP at 5 cm H2O and the antibiotic was changed over to cefoperazone instead of cefotaxime. Child showed clinical improvement with disappearance of cyanosis and the oxygen saturation improved to 97-99%. A chest skiagram at 36 hours of life showed lobar emphysema of the left side with mediastinal shift to right (Fig. 2). Cardiothoracic surgeons were consulted who suggested elective surgery in view of clinical improvement in the child’s condition. The child gradually improved during the next 24 hours and CPAP was withdrawn after 30 hours. Chest skiagram after 3 days was normal (Fig. 3). Blood culture taken at the onset of illness was sterile and the child was discharged after 7 days of antibiotic therapy. The baby is healthy on follow-up.
Lobar emphysema is a rare, life threatening respiratory surgical emergency occurring in neonates. Lobar emphysema refers to abnormal postnatal collection of air within a lobe of the lung that is otherwise normal and is characterized by expiratory air trapping within the affected lung resulting in lobar parenchymal distension. This leads to compression collapse of the surrounding lobes and impaired oxygenation and ventilation(3). Lobar emphysema can occur either due to abnormality of the bronchus or extrinsic or endobronchial obstruction. Congenital lobar emphysema is the result of developmental deficiency of the cartilage that supports the bronchus to the involved lobe, resulting in focal bronchial collapse and obstruction to expiratory airflow. The various lobes involved in congenital lobar emphysema are listed below in the descending order of frequency: left upper lobe (40-50%), right middle lobe (30-40%), right upper lobe (20%) and lower lobes (1%). Endobronchial obstruction can occur due to viscid secretion, mucous plugs or granulation tissue. Vascular anomalies, mediastinal lymph nodes, cysts or tumors can produce extrinsic obstruction(3). Congenital lobar emphysema is characteristically found in term infant, but acquired lobar emphysema is common among preterms(4). The latter problem may result from lung injury related to prolonged ventila-tion and is often associated with broncho-pulmonary dysplasia(2,5). Unlike congenital lobar emphysema, multiple areas of focal hyperinflation and interstitial emphysema are often present. Unilobar right lower lobe involvement is uncommon in acquired lobar emphysema. These characteristics help in differentiating congenital from acquired lobar emphysema. Congenital lobar emphysema has also been described in association with maternal chorioamnionitis and CMV pneumonitis(6,7). The respiratory distress in lobar emphy-sema may be severe needing thoracotomy and resection of the affected lobe. Surgical resection is indicated when the pO2 falls below 50 mmHg and pCO2 rises above 50 mmHg. In lobar emphysema resulting from obstruction due to mucus plug or other secretions, flexible bronchoscopy may be useful for therapeutic and diagnostic purposes. However, some of these children may improve spontaneously like the present case. The present case had pyrexia, respiratory distress and chest radiography suggestive of pneumonia and later lobar emphysema. The presence of pneumonia and secretions could be the cause for airway obstruction and production of lobar emphysema. Though a clinical diagnosis of septicemia was made, surrogate markers of sepsis (µESR, band count) were negative and blood culture was sterile. It is possible that surrogate markers of sepsis and blood culture may not be positive in all cases of septicemia(8). Also this neonate might have had just a pneumonic process without associated septicemia. The unusual features in our case are: (i) occurrence of pneumonia and acquired lobar emphysema in a term infant delivered by elective Caesarean section; (ii) acquired lobar emphysema with unilobar involvement; and (iii) resolution of the condition after positive end expiratory pressure and antibiotic therapy. Contributors: TSV, HR and BVB managed the baby and prepared the manuscript. BVB will act as the guarantor for the paper.
Funding:
None.
|
![]()