|
|
Case Reports Indian Pediatrics 2001; 38: 407-410 |
|||||
|
Non-Hodgkins Lymphoma in a Child Presenting as Nephromegaly and Acute Renal Failure |
|||||
|
Renal masses are commonly encountered clinical problems in children. They could be congenital, inflammatory, traumatic, vascular or neoplastic in origin(1). Among the neoplastic lesions, Wilm’s tumor and renal cell carcinoma are the commonly encountered etiologies. Renal lymphoma is rare and hence not generally considered in the differential diagnosis of renal masses in children(2). It is still rarer for it to present with acute renal failure(3-6). We report here a 4½-year-old boy who presented with this problem.
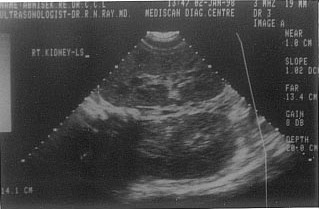
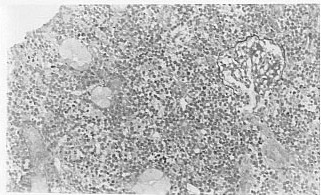
A 4½-year-male child presented with a one month history of progressive distention of abdomen and low grade fever. Since three weeks he also had complaints of swelling over face and feet, vomiting off and on. There was decreased appetite with profuse night sweats since the last 15 days. There was no history of dysuria, hematuria or oliguria or any history of renal disease in the past. Evaluation by the local pediatrician revealed bilateral abdominal lumps in loin with which he was referred to us. On admission, the child appeared ill. He was anemic and there was no icterus. Blood pressure was 102/62 mmHg. Pedal edema was present alongwith mild facial puffiness. There were multiple small (<1 cm) palpable lymphnodes in left axilla (posterior group) and submandibular region. Examination did not reveal any abnormality in respiratory, cardiovascular and central nervous system. On abdominal examination there was no ascites and liver and spleen were not enlarged. Bilateral kidneys were palpable, ballotable with smooth surface and were non tender. Initial investigations revealed: hemoglobin 10 g/dl, peripheral smear normochromic normocytic anemia, leukocyte 4800/mm3, platelet count 2.2 lakhs/mm3, serum creatinine - 2.1 mg/dl, BUN-74 mg/dl, uric acid - 9.4 mg/dl, serum sodium - 138 mEq/L, serum potassium - 4.6 mEq/L, serum bilirubin - 0.3 mg/dl, SGOT - 22 U/L, SGPT 22 U/L, serum total proteins - 6.3 g/dl and serum albumin - 3.4 g/dl. Urine routine examination revealed protein of one plus and microscopy 5-10 WBC/HPF with a spot albumin, creatinine ratio of 0.8. X-ray chest was apparently normal with no evidence of lymphadenopathy. Ultrasound (Fig 1) showed bilaterally grossly enlarged kidneys (bilateral 14 cm in size) with no evidence of hydronephrosis. CT scan (Fig. 2) was done which also revealed bilaterally enlarged kidneys homogeneous in appearance. Renal biopsy was done which revealed extensive tubular and interstitial infiltration by small to medium sized cells displaying round to slightly irregular nuclei containing two or three prominent nucleoli and small amount of deeply staining cytoplasm which tended to square off in places. Frequent mitotic figures and multiple apoptotic bodies were present. Glomeruli were largely unremarkable (Fig. 3). A diagnosis of malignant lymphoma, small-cleaved cell was given. Subsequently, bone marrow examination was done and the findings were suggestive of lymphoproliferative disorder. FNAC of axillary lymph nodes also revealed findings of malignant lymphoma, small non-cleaved cell. CSF examination was also positive for atypical lymphoid cells. Thus a diagnosis of small non-cleaved cell lymphoma (Burkitt’s lymphoma stage IV) was made. Chemotherapy was offered, but in view of the poor prognosis the parents decided against any treatment and took the child home.
Renal involvement in lymphoma is uncommon. It can manifest as nephrotic syndrome secondary to minimal change disease(6,7). Rarely, it may cause nephro-megaly and acute renal failure secondary to a disseminated lymphoma. It is still rare for PRL to present in such a manner. Primary renal lymphoma (PRL) is a controversial and infrequent disease. Some authors believe that since there is no lymphoid tissue in kidneys, a primary renal lymphoma is unlikely. However, others have stated that primary renal lymphoma does occur and also suggested the criteria for diagnosis of this entity(8). Most patients with PRL have no clinical evidence of renal involvement. Extrarenal signs and symptoms of lymphoma are frequently present(9). Thus, the diagnosis of renal lymphoma is often made at autopsy. Obstructive nephropathy was promptly excluded by ultrasonography. The absence of extensive hyperuricemia (serum uric acid >20 mg/dl) and uric acid crystals argues against a diagnosis of uric acid nephropathy. Compression of renal arteries by lymphoma was ruled out by absence of hypertension and the lack of proteinuria is a pointer against a glomerular disease. The presence of massively enlarged kidneys and histopathologic evidence of diffuse lymphocytic infilitration points to primary renal lymphoma as the cause of renal failure(8). Although, this child had evidence of CNS and lymphnode involvement, the renal involvement was out of proportion to that of the other organ systems. Hence, it appears that child had PRL rather than secondary lymphomatous involvement of the kidney. Tissue diagnosis can usually be made by lymph node or bone marrow biopsy in most patients with widespread lymphoma and renal involvement. It is believed that kidney biopsy is the most expeditious and direct way to establish the underlying diagnosis of renal masses besides providing clues to etiology of ARF(1). The prognosis in these patients is usually poor with most patients dying within 9 months of presentation(10). Though a rare entity, PRL should be suspected in any child who presents with bilateral nephromegaly and renal failure and where the radiological imaging excludes obstruction, Wilm’s tumor and renal cell carcinoma. Contributors: AM and SG were involved in care of the patient and preparation of the manuscript. KG was involved in radiological investigations including assistance with USG guided biopsy. MJ was responsible for making the histological diagnosis.
Funding:
None.
|
![]()