|
A
human being is composed of about
1012 cells, which results from approximately 238 mitoses since the moment
of fertilization. During mitosis, cells differentiate into dozens of types
of tissues and organs. This is the actual process of growth and
development(1).
Human growth has been scientifically investigated and
studied since the beginning of science; yet, the exact manner in which a
child grows still remains unanswered. Although remarkable increases in
body size and length occur during organismal growth, very little is known
about the mechanism of the growth process(2).
Longitudinal growth occurs through a process of cell proliferation, the
addition of new cells to the growth plate of the bone and hypertrophy,
resulting in the expansion of the growth plate.
Growth Pattern in Children
Growth of a child was considered to be a relatively
smooth process traditionally–rapid growth during infancy followed by
steady growth in midchildhood and finally the pubertal spurt during
adolescence(3). But studies carried out globally have shown that human
growth is a nonlinear process with marked variation in growth rate during
the short-term. It is not known how long-term height gain or stature is
influenced by short-term changes in height and weight.
|
Daily
empirical observations modeled by several methods describe infant
growth as an aperiodic saltatory or pulsatile process, separated by
variable durations of stasis. |
Daily empirical observations modeled by several methods
describe infant growth as an aperiodic saltatory or pulsatile process,
separated by variable durations of stasis(4). Butler, et al.(5),
after studying the growth velocity data from normal prepubertal children,
described growth spurts over 2-year intervals. Lampl, in 1993, identified
a pattern of growth in the subjects that included intervals of no
significant growth increments, or, stasis, for as long as 1-2 months(6).
It was seen that growth itself occurred during short measurement intervals
that punctuated these stases. These results led to the proposition that
the actual mechanism of growth is a two-phase process–a short time
duration growth of event accompanied by a longer refractory interval, or
stasis. This is what is called as the saltatory model, which defines
growth as a series of rapid growth intervals (saltations) separated by
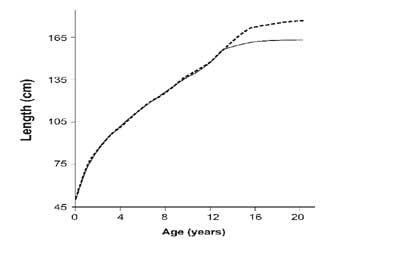
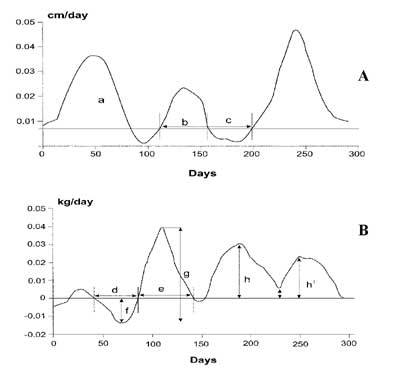
intervals of stasis (Fig. 1)(5,6). Figure 2
represents the schematic explanation of the characteristics of the height
and weight.
 |
|
Fig. 1 Standard growth curves from birth
to 18 years. Data are mathematically smoothed and averaged over
children. Dashed line represents boys. Solid line represents girls.
Adapted from growth charts developed by the National Center for
Health Statistics in collaboration with the National Center for
Chronic Disease Prevention and Health Promotion (2000).
|
 |
|
Fig. 2 Schematic explanation of the
characteristics of the height (A) and weight (B) velocity curves.
Arrowed lines indicate the amplitude of a height velocity peak (a),
length of a height velocity peak (b), and length of a stasis (c) in
A. Length of weight loss (d), length of weight gain (e), amplitude
of weight loss (f), total amplitude of weight velocity (g), and
amplitude of weight gain (h) are shown by arrowed lines in B. If the
minimum between two peaks (i) was less than half of the amplitude of
the smaller peak (h’), then two separate periods of weight gain were
identified. |
Thalange, et al.(7), after studying 46 healthy
prepubertal children showed that the growth in childhood over 1 year is
represented by a biphasic process comprising 3–6 unpredictable growth
spurts, each of mean length 56 days (range 13–155 days), separated by
periods of stasis ( £0.05
cm height increment over more than 7 days), each lasting a mean of 18 days
(range 8–52 days) and accounting for at least 20% of the period of
observation.
|
The growth of children can be considered
continuous when observed across years, with periods of spurts and
stasis. Daily differences in growth may not be visible as growth is
measurable only at certain frequencies. |
It has also been shown that seasonal variations play an
important role in growth increments. There is a declining growth rate over
the autumn months, which reached a nadir in midwinter. This is followed by
a growth spurt in the spring(7). This points out to the fact that human
growth over short periods is a continuous, irregular and unpredictable
process.
The seasonal variation in growth velocity is probably
the most well characterized cyclical pattern of human growth, with peak
velocity in midsummer(8-10). Using knemometry, an accurate and noninvasive
technique of lower leg length measurement, Hermanussen, et al.(11)
showed that lower leg length increased in mini-growth spurts over 30–55
days intervals. In contrast, Lampl, et al.(12) proposed that all
gain in length of normal infants occurred in irregular, brief, 1-day
growth spurts saltations, separated by long periods of growth stasis.
It has also been suggested that the growth process may be governed by the
principles of chaos. Tillman, et al.(13) proposed that height gain
during 1 year is a biphasic process, comprising intense growth spurts
lasting an average 8 weeks, separated by periods of very slow growth or
stasis over 2–3 weeks.
Despite the abundance of adolescent growth studies,
comparatively little is known about sequential development of limb
components and variation in this process. It has been observed that due to
earlier maturation of girls, the length of each of their long bones
exceeds that of boys to some degree during some period of adolescence.
Peak velocities for leg bones occur earlier than those for arm bones, with
the latter more closely coinciding with peak height velocity (peak
velocities (years) females, males: humerus, 11.2, 13.8; radius, 10.7,
13.9; femur, 10.3, 12.7; tibia, indeterminate (linear), 12.4; height,
11.2, 14.0)(14).
The growth of children can be considered continuous
when observed across years, with periods of spurts and stasis. Daily
differences in growth may not be visible as growth is measurable only at
certain frequencies. But there are growth changes happening in the child’s
body during the period of stasis which becomes evident during the period
of growth spurt.
Variations in the Normal Growth Pattern
Although most children follow the normal patterns of
growth, a small number of children have growth patterns that differ from
the typical model. These less common but normal patterns of growth
include:
Growth rate changes in infancy: It is not
unusual for normal children under 2 years of age to cross percentile lines
in either direction. This happens because the factors that affect growth
before birth are different from those that govern growth after birth(15).
Upward or downward shifts: Babies who are small
at birth often shift to a higher growth channel during the first few
months of life, as they ‘catch up’ to their own growth potential. On the
other hand, large or average-size babies who have short parents may have
slower-than-expected growth during the first months of life as they settle
into their own growth channel. A downward shift in growth during the first
1.5–2 years of life may not be a cause for concern if the baby is healthy
and thriving, if he or she has a good diet, and if height and weight are
shifting together(16).
Catch-up growth: The brain regulates the body’s
growth by controlling the feelings of hunger and fullness and makes the
system function to keep each child’s size and shape relatively stable over
the time. During sickness like fever and diarrhea, the quantity of food
and in turn, nutrients consumed by children is less; this results in the
body being depleted of essential nutrients, which makes the immune system
weaker. This results in a lack of growth, both in terms of height and
weight. But once the illness is past, the weight gets back to normal. This
pattern of catch-up growth is a good sign of a healthy body and a healthy
growth-control mechanism(17).
Factors Determining Everyday Growth
What makes one child long and thin, another short and
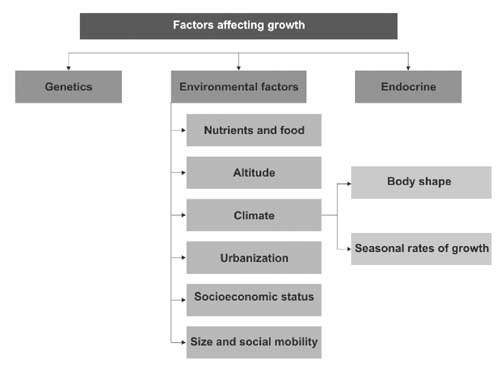
stout? Growth varies with age. Many factors influence how much and how
rapidly a child grows, and how tall he or she will be as an adult (Fig.
3). Some of these factors can be controlled and others cannot. Human
growth rate is determined by a complex interaction of physical, endocrine
and nutritional factors, of which growth hormone (GH) and nutrition are
the key determinants of child growth(1).
 |
|
Fig. 3 Factors affecting growth. |
Heredity or the genetic potential is one of the most
important factors influencing a child’s growth. Growth varies among
different ethnic groups, among different families within the same ethnic
group and even among members of the same family. Growth hormone releasing
hormone stimulates GH pro-duction in the pituitary gland and releases it
into the bloodstream, which in turn helps in the stimulation of IGF-1
resulting in growth. A well-balanced, age-appropriate diet that includes
the essential nutrients especially micronutrients has a positive effect on
how well a child grows(18).
Role of Nutrients in Influencing Growth
Adequate nutrition from fetal stage, in childhood,
during adolescence, pregnancy and lactation is of fundamental importance
for human develop-ment(19). Nutrition is also important for the skeletal
development, which is a part of the growth process. Deficiency of
nutrients can adversely affect the linear growth, cognition and muscle
development. While the role of energy and proteins on physical growth is
well-established, recent studies have stressed on the importance of
micronutrients in enhancing the full growth potential(20). These nutrients
are essential for the assimilation, absorption and utilization of even the
macro nutrients from the daily foods i.e., carbohydrates, proteins and
fats.
Inadequate nutrient intake during childhood leads to
undernutrition, which results in growth retardation, reduced work capacity
and poor mental and social development(21-26). A study carried out by
Satyanarayana, et al.(27) among Indian preadole-scent boys of 5+
years of age for 18 years showed that boys who were nutritionally
deficient were less tall than their counterparts and entered late into
puberty with significantly depressed intensity.
As growth of children can be considered continuous when
observed across years, a daily intake of essential nutrients is necessary
for maintaining this growth. Deficiencies, particularly energy and
micronutrient deficiencies, begins from early fetal life and continues
through childhood, adolescence and reproductive stages of life, resulting
in a vicious cycle of transgenerational events. Strong evidences for iron
and iodine deficiencies compromising cognition and growth are
well-documented. Inadequate nutrient intake will also increase the body’s
susceptibility to infections, which is another causative factor in delayed
or slow growth(28-31).
Only recently is the role of micronutrients in the
etiology of growth is being appreciated. Micronutrient deficiencies
represent a hidden form of hunger with severe consequences on physical
growth, immune functions and cognition. As many of the micronutrients are
water soluble and get excreted, not all of them can be stored in the body.
All of them are not available in required amounts in all the food one eats
everyday.
The effects of deficiencies are multiple and severe in
children and may affect the linear growth, cognition and muscle
development which are often irreversible. While the role of energy and
proteins on physical growth is well-established, a deficiency in the
micronutrient intake may add to the insult. The genetic potential of
children for physical growth and mental development will be compromised
and the susceptibility to infections is increased even in subclinical
deficiencies of multiple vitamins and minerals (Table I).
Children who suffer from malnutrition are more likely to have slowed
growth, delayed development, difficulty in school and high rates of
illness, and they may remain malnourished into adulthood(33).
TABLE I
Role of Micronutrients in Growth
|
Vitamin D and |
Deficiency affects bone development, which manifest as rickets |
|
calcium |
|
|
Potassium, zinc |
Deficiency disturbs the GH/IGF-I system and affects growth |
|
magnesium and copper |
|
Manganese
|
Deficiency leads to skeletal abnormalities including
retarded growth, which may be mediated through detects in
proteoglycan physiology in the growth plate |
| Iron and iodine |
Helps in cognitive development and growth |
| Vitamin A |
Indirectly helps in growth |
| Zinc |
Overall growth |
| Vitamin E |
Muscle development |
Studies have shown that the nutrient intake, especially
the micronutrient intake of Indian school going children do not meet the
Recommended Dietary Allowances suggested by Indian Council of Medical
Research. Countrywide surveys conducted by the National Nutrition
Monitoring Bureau (NNMB, 1998) showed that Indian diets were qualitatively
adequate in proteins but deficient in some micronutrients. Thus, if
caloric needs are met, protein requirements too are fulfilled, but the
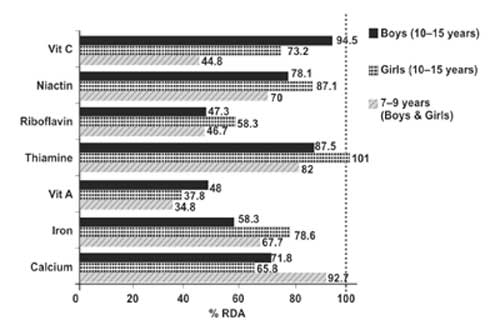
requirement of several micronutrients (Fig. 4) remains
unmet. Since Indian diets have not changed substantially over the years,
these observations apply even today. While dietary deficiencies of vitamin
A and riboflavin are seen in all age, sex and physiological groups, those
of other micronutrients, such as iron, calcium, thiamine, niacin and
vitamin C are seen high in children(34).
 |
|
Fig. 4 Graph depicting the micronutrient
intake of Indian children (Boys and girls) in the age group of 7-15
years as compared to 100% RDA as per NNMB 1996 Data. (RDA marked as
dotted line). |
Gaps in Indian Diet
A study carried out recently by the National Institute
of Nutrition showed that subclinical micronutrient deficiencies among
those who have adequate protein and calorie intake may be an important
contributing factor for not achieving the growth potential. The study was
carried out in semi-urban middle-income residential schoolchildren aged
6–16 years(35). It was observed that the extent of inadequacy at baseline
was almost 100% for folic acid, 65% for vitamins B 2
and B6 and 55% for vitamin C and 44% for vitamin A. The
prevalence of anemia among subjects was 54%, with inadequacy of vitamin B12
being 40% and that of vitamin D being 30%(36).
Ensuring Optimal Nutrient Intake
Prevention against growth failure and ensuring full
growth potential is therefore, of primary importance and is possible at
several stages of life through focused approaches. Assuring adequate
nutrient intake is one approach to prevent and overcome growth failure
problems. We have moved away from protein gap to energy gap and currently
our focus of attention is on micronutrient deficiencies as impediments for
linear growth(37).
However, it is seen that the children are not taking
the required vitamins and minerals on a daily basis. Fast foods are
gaining an upper hand over conventional foods resulting in
multimicronutrient deficiencies. The high activity level of children
coupled with the frequent childhood infections, their life style to
withstand the competition, in the prevailing environment of urbanization
and globalization further increase the nutrients required, which call for
the need for more nutrients in addition to that from their diet.
Several approaches may be taken to improve the intake
of growth-promoting nutrients, including daily administration of
micronutrient supplements, forti-fication of food with micronutrients or
improved dietary intake on a daily basis.
Role of Nutritional Supplements in Children
Bioavailability of the nutrients, especially that of
the micronutrients, are reduced due to factors like the nature of Indian
diet, cooking methods followed and high prevalence of fast food
consumption among children. Hence, one cannot be really sure about the
particular nutrients children derive from their food, owing to the loss of
nutrients as a result of cooking and due to the presence of preservatives,
colors and pesticides. As growth may be affected by more than one
growth-limiting nutrient, intervention studies focus on the importance of
multiple micronutrients. Hence, in ensuring adequate nutrient intake,
multimicronutrient supplementation is essential in addition to food on a
daily basis.
• Nutritional intake plays a major role in the
performance at school and in the general understanding and retention
capacity of the students.
• Well-nourished children not only are better
physically but also mentally(38).
Meta-analyses of studies conducted to assess the
effects of vitamin A, iron and multimicronutrient interventions on the
growth of children <18 years showed that interventions limited to only
vitamin A or iron did not improve child growth. Multi-micronutrient
interventions on a daily basis, on the other hand, improved linear and
possibly ponderal growth in children(39).
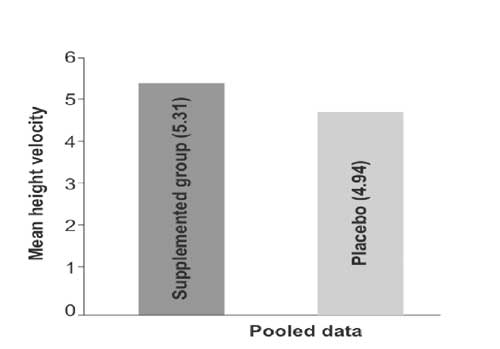
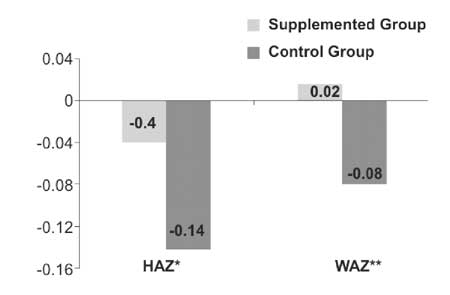
Bhandari, et al.(40) examined the impact of
daily multimicronutrient supplementation on linear growth either singly or
in combination for various age groups such as infants, preschoolers and
school going children. Single nutrients did not impact linear growth. Zinc
supplements had a small effect on length (0.22 SD units) in children of
0–13 years of age. Sarma, et al.(41) in a double-blind
placebo-controlled, matched paired, cluster randomized study in children
aged 6–16 years after 14 months of multimicronutrient rich beverage
administration on a daily basis observed a significant increase in mean
increments of height and weight Z scores of 0.04 and 0.02,
respectively. Velocity of weight (3.56 vs. 3.0) was also significantly
higher in supplemented group. In this study, the usual diets provided 80%
of their energy requirements (Figs. 5 and 6)(41).
 |
|
Fig. 5 Height velocity. |
 |
|
Fig. 6 Mean Z-scores of increments in
height and weight in the study groups. HAZ, height-for-age Z score;
WAZ, weight-for-age Z- score. *P=0.016. **P=0.002. |
Conclusion
Growth in children can be considered continuous when
observed across years with periods of spurts and stasis. Daily differences
in growth may not be visible as growth is measurable only at certain
frequencies. However, there are growth changes happening in the child’s
body even during the period of stasis which become evident during the
growth spurt. Hence, adequate nutrition is required everyday for normal
growth to happen.
Data shows that the typical Indian diet does not
provide adequate quantity of all essential micronutrients. Further,
studies have conclusively shown that daily micronutrient supplementation
improved height even in apparently healthy children. Hence, it can be
concluded that the process of growth happens on a daily basis; therefore
it becomes critical to provide all key micronutrients in adequate
quantities to children on a daily basis.
Funding: None.
Competing interests: None stated. Conclusions in
this Perspective are those of author and do not necessarily represent the
views of the funding agency.
References
1. Bogin B. Patterns of Human Growth. London: Cambridge
University Press; 1999.
2. Johnson ML, Veldhuis JD, Lampl M. Is growth
salutatory. The usefulness and limitations of frequency distributions in
analyzing pulsatile data. Endocrinology 1996; 137: 5197-5204.
3. Malina RM. Motor development during infancy and
early childhood: Overview and suggested directions for research. Int J
Sport Health Sci 2004; 2: 50-66.
4. Michelle L, Johnson ML. Identifying saltatory growth
patterns in infancy: A comparison of results based on measurement
protocol. Am J Hum Biol 1997; 9: 343-355.
5. Butler GE, McKie M, Ratcliffe SG. The cyclical
nature of prepubertal growth. Ann Hum Biol 1990; 17: 177-198.
6. Lampl M. Evidence of saltatory growth in infancy. Am
J Hum Biol 1993; 5: 641-652.
7. Thalange NKS, Foster PJ, Gill MS, Price DA, Clayton
PE. A model of normal prepubertal growth. Arch Dis Child 1996; 75:
427-431.
8. Fitt AB. Seasonal Influence on Growth Function and
Inheritance. Wellington: New Zealand Council for Educational Research;
1941.
9. Bransby ER. The seasonal growth of children. Med
Officer 1945; 73: 149-165.
10. Marshall WA. Evaluation of growth rate in height
over periods of less than one year. Arch Dis Child 1971; 46: 414-420.
11. Hermanussen M, Geiger-Benoit K, Burmeister J,
Sippell WG. Periodical changes of short-term growth velocity (‘mini growth
spurts’) in human growth. Ann Hum Biol 1988; 15: 103-109.
12. Lampl M, Veldhuis JD, Johnson ML. Saltation and
stasis: A model of human growth. Science 1992; 258: 801-803.
13. Tillman V, Thalange NKS, Foster PJ, Gill MS, Price
DA, Clayton PE. The relationship between stature, growth and short-term
changes in height and weight in normal prepubertal children. Pediatr Res
1998; 44: 882-886.
14. Smith SL, Buschang PH. Longitudinal models of long
bone growth during adolescence. Am J Hum Biol 2005; 17: 731-745.
15. Manly T, Cornish K, Grant C, Dobler V, Hollis C.
Examining the relationship between rightward visuo-spatial bias and poor
attention within the normal child population using a brief screening task.
J Child Psy Psychiatry 2005; 46: 1337-1344.
16. Vogiatzi MG, Copeland KC. The short child. Pediatr
Rev 1998; 19: 92-99.
17. Adair LS. Filipino children exhibit catch-up growth
from age 2 to 12 years. J Nutr 1999; 129: 1140-1148.
18. Eveleth PB, Tanner JM. Worldwide Variation in Human
Growth. Cambridge: Cambridge University Press; 1990.
19. The World Health Report 2002. Reducing risks,
promoting healthy life: Overview, Geneva, World Health Organisation, 2002
(WHO/WHR/02.1).
20. Graham GG. Environmental factors affecting the
growth of children. Am J Clin Nutr 1972; 25: 1184-1188.
21. Sandstead HH, Penland JG, Alcock NW, Dayal HH, Chen
XC, Li JS, et al. Effects of repletion with zinc and other
micronutrients on neuro-psychologic performance and growth of Chinese
children. Am J Clin Nutr 1998; 68: S470-S475.
22. Harahap H, Jahari AB, Husaini MA, Saco-Pollitt C,
Pollitt E. Effects of an energy and micronutrient supplement on iron
deficiency anemia, physical activity and motor and mental development in
undernourished children in Indonesia. Eur J Clin Nutr 2000; 54: S114-S119.
23. Bates CJ, Evans PH, Allison G, Sonko BJ, Hoare S,
Goodrich S, et al. Biochemical indices and neuromuscular function
tests in rural Gambian school children given a riboflavin, or multivitamin
plus iron supplement. Br J Nutr 1994; 72: 601-610.
24. Bamji MS, Sarma KVR, Radhaiah G. Relationship
between biochemical and clinical indices of B-vitamin deficiency in rural
school boys. Br J Nutr 1979; 41: 431-440.
25. Sarma KVR, Radhaiah G, Bamji MS. Impact of long
term low dose supplementation of B-complex vitamins on clinical and
anthropometric status of rural school children. Nutr Rept Int 1981; 24: 2.
26. Bamji MS, Arya S, Sarma KVR, Radhaiah G. Impact of
long term low dose supplementation of B-complex vitamins on biochemical
and psychomotor status of rural school children. Nutr Res 1982; 2:
147-153.
27. Satyanarayana K, Radhaiah G, Mohan KR, Thimmayamma
BV, Rao NP, Rao BS, et al. The adolescent growth spurt of height
among rural Indian boys in relation to childhood nutritional background:
An 18 year longitudinal study. Ann Hum Biol 1989; 16: 289-300.
28. Gibson RS, Hotz C. Nutritional causes of linear
growth faltering in infants during the complementary feeding period. In:
Martorell R, Haschke F, editors. Nutrition and Growth. Nestle Nutrition
Workshop Series No. 2006; 47: 159-192.
29. Bhan MK, Bahl R, Bhandari N. Infection: How
important are its effect on child nutrition and growth. In:
Martorell R, Haschke F, editors. Nestle Nutrition Workshop Series 2006;
47: 197-222.
30. Brown KH, Peerson JM, Rivera J, Allen LH. Effect of
supplemental zinc on the growth and serum zinc concentrations of
prepubertal children: A meta-analysis of randomized controlled trials. Am
J Clin Nutr 2002; 75: 1062-1071.
31. Rivera JA, Hotz C, Gonzalez-Cossio T, Neufeld L,
Garcia-Guerra A. The effect of micronutrient deficiencies on child growth:
A review of results from community-based supplementation trials. J Nutr
2003; 133: 4010S-4020S.
32. Tandon N, Marwaha RK, Kalra S, Gupta N, Dudha A,
Kochupillai N, et al. Bone mineral parameters in healthy young
Indian adults with optimal vitamin D availability. Natl Med J India 2003:
16: 298-302.
33. Bhan MK, Sommerfelt H, Strand T. Micronutrient
deficiency in children. Br J Nutr 2001; 85: S199-203.
34. Brahmam GNV. National Nutrition Monitoring Bureau
in India: An overview. Indian J Comm Med 2007; 32: 5.
35. Sivakumar B, Vijayaraghavan K, Vazir S, Balakrishna
N, Shatrugna V, Sarma KV, et al. Effect of micronutrient supplement
on health and nutritional status of schoolchildren: Study design.
Nutrition 2006; 22: S1-S7.
36. Sivakumar B, Nair KMN, Sreeramulu D, Suryanarayana
P, Ravinder P, Shatrugna V, et al. Effect of micronutrient
supplement on health and nutritional status of schoolchildren: Biochemical
status. Nutrition 2006; 22: S15-S25.
37. Allen LH. Interventions for micronutrient
deficiency control in developing countries: Past, present and future. J
Nutr 2003; 133: 3875S-3878S.
38. Vazir S, Nagalla B, Thangiah V, Kamasamudram V,
Bhattiproulu S. Effect of micronutrient supplement on health and
nutritional status of schoolchildren: Mental function. Nutrition 2006; 22:
S26-S32.
39. Ramakrishnan U, Aburto N, McCabe G, Martorell R.
Multimicronutrient interventions but not vitamin A or iron interventions
alone improve child growth: Results of 3 meta-analyses. J Nutr 2004; 134:
2592-2602.
40. Bhandari N, Taneja S, Mazumder S, Bahl R, Fontaine
O, Bhan MK, et al. Zinc Study Group. Adding zinc to supplemental
iron and folic acid does not affect mortality and severe morbidity in
young children. J Nutr 2007; 137: 112-117.
41. Sarma KVR, Udaykumar P, Balakrishna N,
Vijayaraghavan K, Sivakumar B. Effect of micronutrient supplementation on
health and nutritional status of schoolchildren: growth and morbidity.
Nutrition 2006; 22: S8-S14. |


