|
|
Case Reports Indian Pediatrics 2001; 38: 1052-1055 |
||
|
Neonatal Hepatic Hemagioendothelioma: Unusual Presentations |
||
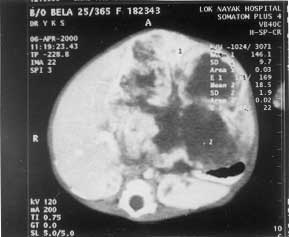
Infantile hepatic hemangioendothelioma is a rare benign vascular tumor that presents most commonly before the age of 6 months. It presents as an abdominal mass with or without congestive cardiac failure. We present two neonates, one presenting with gastric outlet obstruction and the other detected antenatally but with no clinical signs after birth. Case Reports Case 1 A 25-day-old female child weighing 2.3 kg presented with complaints of a progressively increasing abdominal mass since birth, intolerance to feeds and recurrent nonbilious vomiting since one week. On examination, the child was anicteric and had a pansystolic mur-mur. There was a lobulated mass occupying most of the abdomen measuring 10×10 cm. It moved with respiration and auscultation over the mass revealed no bruit. Routine blood examination and liver function tests were normal. The chest roent-genogram was normal. Abdominal sonography revealed a mass arising from the left lobe of the liver. The CT scan of the abdomen showed a heterogeneous soft tissue mass extending from upper abdomen to almost the pelvic inlet. The mass contained both hypodense areas (suggestive of tumor necrosis) and enhancing hyperdense areas with small calcific foci. The mass displaced the stomach posteriorly and caused gastric outlet obstruction (Fig. 1).
In view of the features of gastric outlet obstruction and an inability to accept feeds, an emergency exploratory laparatomy was done. A large lobulated tumor arising from the left lobe of the liver was noted; it was pressing on the pyloric region of the stomach. Left hemihepatectomy using a ball-tipped electro-cautery was performed. The resected specimen showed the tumor involving the whole of left lobe with the cut surface showing solid areas interspersed with areas of necrosis. The histopathology was suggestive of a hepatic hemangioendotheli-oma. Postoperative recovery was uneventful. The patient was reviewed three months after surgery. She had gained weight and ultra-sonography showed evidence of liver regeneration. Case 2 A male child was born to a 34-year second gravida with an antenatal diagnosis of an echogenic mass (5×3.5×3.5 cm) in relation to the left lobe of liver. The child was born of a normal vaginal delivery weighing 3.7 kg. Examination did not reveal any cutaneous hemangiomas or features of congestive cardiac failure. The child was anicteric, had mild hepatomegaly; although no distinct mass could be appreciated. The postnatal ultrasonography of the abdomen showed a well defined bilobed echogenic mass lesion measuring 5.2×3.2×4.2 cm in liver parenchyma involving mainly the caudate lobe and the right lobe of the liver. The mass was displacing the portal vein anteriorly and was pressing on the inferior vena cava. There was no free fluid or lymph nodes. The alpha-fetoprotein level on day two of life was (43567 ng/ml). The MRI of the patient revealed a large well-defined lobulated mass involving the caudate and the right lobes with extension into the left lobe as well, measuring 5.1×2.9 cm. It was hyper intense on T2 weighted and hypo intense on T1 weighted images. Both kidneys and the adrenals were normal. These findings were suggestive of a hemangio-endothelioma of the liver. The patient is under close follow-up. Discussion Hepatic hemangioendothelioma (HHE) is a rare, benign tumor that appears during the first six-months of life. Considered the most common vascular tumor of the liver in children, it is associated with a high mortality rate. HHE can be associated with congestive heart failure, anemia, thrombocytopenia (Kasabach-Merritt syndrome), hepatomegaly and cutaneous hemangiomas. The presentation of a HHE with recurrent vomiting and gastric outlet obstruction is rarely mentioned. However, a comprehensive review of the available literature revealed that one out of eight patients had vomiting or feeding abnormalities as an associated feature. Only one case hitherto has been reported having vomiting as the main presenting feature(1); the neonate had bilious vomiting and an abdominal lump and the preoperative diagnosis of duodenal stenosis with a possible midgut volvulus was enter-tained. On exploration, the hemangiomatous tumor was found to be pressing onto the third part of the duodenum. Prenatal diagnosis has been associated with hydrops fetalis(2). Postnatal diagnosis is established with US, CT scan and MRI. MRI is the preferred investigation as it can accurately define the extent and nature of this vascular lesion obviating the need of a diagnostic arteriography(3). Biopsy is not advised as it may result in massive hemmorrhage. Traditionally, serum alpha-fetoprotein levels have been used as tumor markers for hepatoblastoma and had often been used to differentiate hepatoblastoma from HHE. But a few recent reports suggest that even cases of HHE may be associated with massively elevated levels(4,5). Elevated maternal levels of alpha-fetoprotein have also been seen with cases of fetal hepatic hemangioendothe-lioma(6). Natural history of asymptomatic HHE is spontaneous involution and no treatment is required in incidentally discovered case. Symptomatic lesions need aggressive manage-ment. Radiotherapy and chemotherapy have not shown consistently good results. Steroid(7) and alpha-interferon(8) are used as initial treatment to inhibit proliferation of endothelial and smooth muscle cells. Symptomatic solitary lesions can be managed with resection. Severe bilobar disease might need hepatic artery embolization(9) or liver transplantation. Hepatic artery ligation or embolization should not be done in patients with shunting from the portal vein to the hepatic vein and minimal systemic arterial collateral circulation, since it can result in hepatic necrosis. Hepatic resection has been traditionally recommended only for the management of rupture with hemorrhage or for the treatment of a localized tumor that is indistinguishable from malignant disease. There has been a growing recent trend in certain specialized centers to opt for a surgical excision in cases of symptomatic hemangioendothelioma(10). Our experience in the first case provides further evidence that localized tumors can be safely excised even in moderate setups. By adopting this modality of therapy, we could avoid the long period of parenteral nutrition with its attendant complications. Contributors: AS, SR and YKS contributed to the drafting of the paper. SR and YKS were involved in the management of the patients.
Funding: None
| ||
| References | ||
|
![]()