|
|
Case Reports Indian Pediatrics 2001; 38: 949-951 |
||
|
Schizencephaly Type-I |
||
|
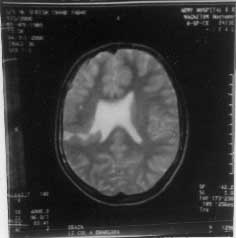
Amongst the cortical malformations, schizencephaly is more severe, yet restricted disorder(1,2). The lesion may be suspected by the appearance of focal ventricular dilatation on ultrasonogram and by visualization of gray matter lined cleft on CT Scan(3,4). However, the most sensitive modality for demonstration of schizencephaly is MRI(3,5). Of the two types of the schizencephaly described, Type I which consists of fused cleft without hydro-cephalus may not be detected by sonography, but is readily identified by CT/MRI(6,7). We report a case of Type I Schizencephaly for its rarity and to highlight sensitivity of MRI in demonstrating the lesion. Case Report An 11-year-old male child elder of the two siblings, was born at term to non-consan-guineous parents. Antenatal, intranatal and perinatal periods were uneventful. He pre-sented with global delay of motor milestones, frequent falls and weakness of the left half of the body since early infancy. There was no history of seizures. Scholastic performance of the child was within normal limits. Investigation profile revealed normal blood count and hematocrit. Screening for tuberculosis was negative. Relevant tests to exclude collagen disorder were within normal limits. There was no evidence of hemolysis. Echocardiography and electroencephalogram were normal. CT scan cranium showed a cleft in right temporo-parietal region; however, communication of the cleft could not be delineated. MRI (Fig. 1) showed a prominent cleft in right temporo-parietal region cleaving the right parietal lobe, extending from cerebral convexity to right lateral ventricle. There was no communication with the ventricular system. Heterotopic gray matter was seen lining the cleft.
Fig. 1. MRI showing a prominent cleft in right temporo-parietal region cleaving the right parietal lobe, extending from cerebral convexity to right lateral ventricle. There was no communication with the ventricular system. Heterotopic gray matter lining the cleft can be seen. Discussion Schizencephaly is a disorder characterized by a cleft in cerebral mantle, which commu-nicates between the subarachnoid space laterally, and ventricular system medially. The disorder was originally described by Yakovlev and Wadswoth(1,2). They described two variants of Schizencephaly by the presence of "fused" cleft in cerebral mantle (Type I) as opposed to separated cleft or mantle with concordant "Hydrocephalus" (Type II). Schizencephaly is an extremely rare disorder. In literature approximately 70 cases of Type II Schizencephaly have been reported(8,9). The exact incidence of Type I Schizencephaly is not known. In a study of 20 MRI confirmed cases of Schizencephaly, 50% were of closed lip type (Type I) and the lesions were unilateral in 65% cases(5). The exact etiopathogenesis of Schiz-encephaly is unknown. The original work of Yakovlev and Wadsworth contends that the failure of normal migration of the primitive normoblasts results in the cerebral cleft(1,2). In the walls of the cleft the cerebral mantle exhibits the hallmarks of the migrational disturbance, e.g., thick microgyri, cortex and large neuronal heterotopias as seen in the MRI of our case also(10). The continuity of the gray matter along the associated cerebral malforma-tion supports this theory(6). Others contend that Schizencephaly is a part of spectrum of encephaloclastic dis-order(11). In utero, sonographically detected progressive destructive changes of vascular insult in the distribution of the middle cerebral artery territory in a case of Schizencephaly add support to the hypothesis of encephaloclastic theory(8). Other workers have also hypo-thesized a vascular etiology. They proposed that the abnormality results from an infarc- tion in area of the germinal matrix during the seventh week of embryogenesis. Their theory is based on the demonstration of a watershed zone in the gray matter along the lateral ventricle in the area of the germinal matrix(12). There is also evidence suggesting that unilateral Schizencephaly can be familial and probably accounts for previously reported "familial porencephaly"(13,14). Recent studies using Single Strand Conformation Polymorphism (SSCP) have revealed germline mutation in the homebox gene EMX2 in patients with severe Schiz-encephaly(15-17). However, different mor-phoclinical pictures of Schizencephalics suggest that besides EMX2 mutation, other factors are also relevant in determining the severity of the brain malformation and the clinical picture(17). In view of clinical and radiological profile, a diagnosis of Type I Schizencephaly was made. The cardinal neuropathological features of Schizencephaly are: (i) Hemispheric cleft lined by piaependyma usually bilateral in the area of Sylvian fissure; (ii) Communication of the subarachnoid space with the lateral ventricle medially with infolding of the gray matter along the cleft; and (iii) Multiple associated intracranial malformations including poly-microgyria, gray matter hetertopias, absent septum pellucidum, optic nerve hypoplasia and agenesis of corpus callosum(1,8). Ultrasonographic (USG) diagnosis depends upon the demonstration of defect in the cerebral mantle in the area of Sylvian fis-sure and establishing communication between enlarged lateral ventricle and subarachnoid space. It can also demonstrate associated cerebral malformations such as absent septum pellucidum and agenesis of corpus callo-sum(8,9). USG may be of help in differ-entiating Schizencephaly from other condi-tions that have appearance of CSF filled spaces, e.g. holoprosencephaly, porencephaly, hydra-nencephaly, subarachnoid cysts, etc. In Type I variety which consists of fused cleft without hydrocephalus, USG may not be able to detect the schizencephalic cleft which can only be detected by CT/MRI(6,7). Since MRI is a new imaging modality and is not widely available, further studies will be required to assess the true prevalence of this disorder and to evaluate the structural defects in Type I schizencephalics. Contributors: AKD conceived the idea and co-drafted the manuscript. He will act as the guarantor for the paper. RKG assisted in writing the manuscript. PS helped in imaging. RKS assisted in writing the manuscript. Funding: None.
| ||
| References | ||
|
![]()