|
|
Case Reports Indian Pediatrics 2000;37: 1005-1009 |
||||||||
|
Chorea: An Unusual Presenting Feature in Pediatric Moyamoya Disease |
||||||||
|
Moyamoya disease is a rare disease characterized by multiple occlusions of the cerebral circulation with an unusual net like system of collaterals. In Japanese, Moyamoya means ‘hazy’. The disease derives its peculiar name from the angiographic appearance of cerebral vessels in the disease that resembles a ‘puff of smoke’. In children the most common presentation is that of recurrent episodes of cerebral ischemia manifesting clinically as focal deficits, parasthesiae and seizures(13). Two cases of Moyamoya disease with uncommon present-ing features are described here.
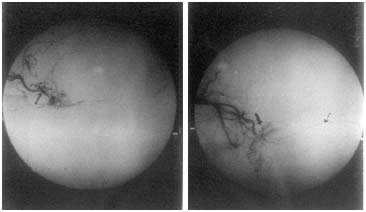
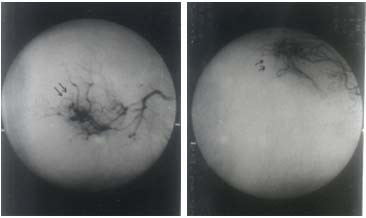
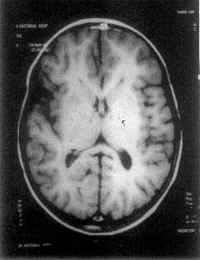
Case 1: An 11-year-old male child presented with complaints of unsteadiness of gait and scholastic problems for the last 1½ years. His complaints were static with no history of seizures, focal deficits or sensory involvement. His examination was unremarkable except for chloreiform movements involving the left upper and lower limbs. On examination, milk-maid's sign and pronator sign could be demonstrated on the left side. MRI showed focal hyperintense lesions in the periventricular white matter of both the hemispheres and focal areas of signal abnor-malities in both centrum semiovale, periventri-cular white matter, right parietal cortex and subcortical white matter. MRI angiography showed that the supra-clinoid segments of both the internal carotid arteries (ICA) were narrowed, the middle and anterior cerebral arteries (MCA and ACA) were thin and the extensive basal collaterization gave rise to the characteristic ‘moya’ formation. The vertebrobasilar system was normal. Antistreptolysin-O (ASO) titer was normal and sickling test and tests for antinuclear antibodies in blood and homocysteine in urine were negative. Hematological work-up which included estimation of Russel viper venom time, Kaolin clotting time and determination of Activated protein-C resistance were normal. Mantoux test was negative and there was no clinical or radiological evidence of a tuberculous lesion. While awaiting surgical intervention, the patient developed right sided hemiparesis. Pre-operative digital substraction angio-graphy (DSA) revealed the classical pattern of progressive vasculopathy as seen in moyamoya disease with partial reformation of anterior circulation through the vertebro-basilar system (Fig. 1). The patient underwent encephaloduro-arteriosynangiosis in the form of left superficial temporal artery (STA)-middle cerebral artery (MCA) onlay 15 days after the onset of the hemiparesis. After this surgical intervention the hemiplegia improved over the next two months. Seven months following surgery, the patient was re-evaluated. His deficits had all but disappeared, chorea had decreased and no new episodes of neurologic deficits had occured. DSA done at this follow-up visit revealed good revascularisation of MCA territory from STA (Fig. 2). It also showed retrogade filling of ACA through MCA. The patient then underwent surgery on the right side. Case 2: A 9-year-old female child presented with choreiform movements involving both upper and lower limbs for 15 days. There was no history suggestive of rheumatic fever in the past nor was there any past history of seizures, scholastic problems and focal deficits. On examination, she was noticed to have spasticity, brisk tendon reflexes bilaterally with bilateral choreiform movements. MRI demonstrated lacunar infarcts involv-ing the basal ganglia (Fig. 3), corona radiata and centrum semiovale with possible narrowing of the supraclinoid and intracavernous portions of the ICA, bilaterally. MRI angiography confirmed the presence of narrowing of the internal carotid arteries and also revealed multiple tortuous collaterals in the supracellar region. The digital subtraction angiography showed total occlusion of the supraclinoid portion of both the ICAs, presence of distal collaterals and bilateral extensive collaterals from meningeal vessels supplying the brain via the durapial anasto-moses. The vertebrobasilar circulation was normal. These findings were characteristic of Moyamoya disease. There was no clinical or radiological evidence of tuberculosis. Mantoux test was negative. Sickling test and test for homocysteine in the urine was negative. The kaolin clotting time and test for activated protein C resistance were also normal. She has under-gone encephaloduroarteriosynangiosis in the form of STA-MCA onlay.
Fig. 1. Pre-operative DSA showing common carotid arterio-gram. Dotted arrow points to STA, not supplying the MCA territory. Dark arrow points to moyamoya formation. Small arrow indicates narrowing of supraclinoid portion of ICA.
Fig. 2. Post-operative DSA showing external carotid arteriogram. Arrow points to successful revscularisation of MCA through STA. STA: Superficial temporal artery. MCA: Middle cerebral artery. ICA: Internal Carotid Artery.
Fig. 3. T2 weighted image of MRI-Brain. Arrow points to lacunar infarcts seen in the basal ganglia region.
In children, Moyamoya disease presents with symptoms suggestive of ischemia of the brain. These usually include episodes of migraine-like headaches, seizures, focal neurological deficits, recurrent strokes or alternating hemiplegia. Involuntary movements have been rarely described previously(4,5). As the disease occurs as a result of progressive occlusion of the intracranial internal carotid arteries and to a lesser degree the proximal anterior and middle cerebral arteries, occurrence of basal ganglia infarcts and chorea can be explained. In developing countries, rheumatic fever is highly prevalent and rheumatic chorea (St. Vitus dance) is considered in the differential diagnosis of any case of chorea. As chorea is a late manifestation of rheumatic fever, no other features enlisted in the Jones’ criteria may be present at the time, the chorea presents itself. In such situations, the physician could be tempted to make a diagnosis of rheumatic chorea without undertaking any further evaluation. Our patients who presented with chorea did not have previous history of hemiplegia, monoplegia or transient ischemic attacks that could have suggested the presence of a vascular etiology. Although, Case 2 did have long tract signs that pointed to multifocal cerebral involvement, cases of Moyamoya disease presenting with chorea alone have been described(4,5) as seen in Case 1. In the absence of any plausible explanation for involuntary movements, it is prudent for a physician to go ahead with neuroimaging studies. Computerized tomography in a case of moyamoya disease may reveal the presence of infarcts, cerebral cortical atrophy or intracranial hemorrhage. It may also show the presence of abnormal collateral vessels in the basal ganglia that enhance after the injection of an intravenous contrast. However, these changes do not provide conclusive evidence of Moyamoya disease. MRI and MR angiography (MRA) with their ability to demonstrate intracranial vessels without the need of potentially toxic intravenous contrast medium have been proposed as the first line investigations in cases of suspected Moyamoya disease(6,7). Although, MRA is more specific than MRI in delineating the course and affection of intracranial vessels, its availaility is limited. Findings such as lacunar infarcts in basal ganglia (as in Case 2) can serve as indirect pointers to the presence of a diffuse vascular affection as seen in Moyamoya disease. Such affection of basal ganglia can explain the presence of chorea (Case 2). Arteriography has traditionally been regarded as essential for definitive diagnosis of moyamoya disease. But MRI and MRA may soon substitute it as a diagnostic test. Arteriography, however, may be required to delineate the extent of collateral flow provided by the vertebro-basilar and external carotid arterial systems(8,9). It should, however, be remembered that Moyamoya disease refers to just an angio-graphic pattern of cerebral vessels and can occur due to a variety of conditions like tuberculosis, fibromuscular dysplasia, neurofibromatosis and sickle cell disease, amongst others(10). Recently, a gene mapping to chromosome 3p which is responsible for familial variety of Moyamoya disease has also been identified(11). Surgical intervention remains the mainstay of the treatment. Various surgical revascularisation options such as multiple burr holes, encephalo-duroarteriosynangiosis, encephaloduroarterio-myosynangiosis and anastomosis between superficial temporal artery (STA) and MCA or ACA have been described(12,15). These procedures are of proven benefit in pediatric Moyamoya disease(12,14,16). It is, therefore, important to be aware of typical as well as unusual presentations of this disease so that surgical intervention can be undertaken early, before irreversible damage occurs.
Authors thank Dr. R.G. Shirahatti, Dean, Seth G.S. Medical College and K.E.M.Hospital for permission to publish the report. Contributors: RP collected the data, assisted in literature search and drafted the paper. SBB edited the draft. He will act as the guarantor for the paper. MNM performed the literature search, drafted the paper and assisted in editing the paper. UL participated in data colection and assisted in drafting the paper. Funding:
None.
|
![]()