angaroo Mother Care (KMC) is widely recognized as
an excellent intervention for improving the health and survival chances
of premature and low-birthweight infants. KMC consists of early,
continuous and prolonged skin-to-skin contact between the caregiver and
the baby, exclusive breastfeeding or breastmilk, and context-appropriate
discharge and follow-up provided to the baby and his or her family [1].
The last 20 years were passed generating and
presenting evidence for utility of KMC in the scientific literature [2].
Globally, 15.5% of all births are LBW babies – with higher proportion in
low- and middle-income countries [3]. Survival chances are less beyond
first year and the survived have significantly high risk to develop
long-term health problems including sensory deficit and
neurodevelopmental disabilities [4,5]. Not only it has shown reduced
neonatal mortality, good school performances have been observed in
preterm who has received KMC [6]. Early initiation and prolonged
skin-to-skin contact has shown tremendous benefits.
Almost 25 years ago, following their visit to
Colombia, a few pediatricians from India initiated KMC practice in
handful units across India [7]. In the past few years, KMC has attracted
even more attention, with an International Kangaroo Mother Care
conference held at Ahmedabad in 2012, a Kangaroo Mother Care Foundation
being set up in India, and greater attention by the government of India
and UNICEF towards promoting KMC across neonatal units [8].
Two studies have shown neonates receiving only a
measly number of hours of KMC. In a paper published in 2015, a
KMC-friendly unit had about four hours of KMC on an average [9], while
in another paper, it was noted that private pediatricians abandoned KMC
on the introduction of EMBRACE [10].
Requirements for KMC Implementation [11,12]
A hospital should allow 24×7 access to the parents to
the neonatal unit at all times. A room near to or at the neonatal unit,
furnished with comfortable seats for the mothers should also be ensured.
Reclining chairs in the nursery and postnatal wards, and beds with
adjustable backrest should be arranged. Mothers can provide KMC sitting
on an ordinary chair or in a semi-reclining posture on the bed with help
of pillows. Appropriate supporting staff and a nurse trained in
assisting mothers in KMC should be available round the clock. All
nursing staff should receive adequate training on KMC, including
nutrition of LBW infants, expression and storage of breast milk, using
alternate methods of feeding and daily growth monitoring of LBW infants.
Educational material such as information sheet, posters, and video films
on KMC in local language should be available to the mothers, families
and the community.
While we have evidence on the beneficial effects of
KMC, along with its incorporation in training content, and a Government
of India policy document related to KMC; we still lag in the adequate
utilization of KMC as a tool for reduction of neonatal mortality rate.
Problems Related to Lack of Implementation
Despite available literature on KMC from India, there
is still a lack of a well-conducted study that describes reasons for not
implementing KMC for neonates that are eligible. Literature from other
parts of the world suggests that it may be due to a host of causes (Box
1) [13-15].
|
Box 1 Problems Faced During
Implementation of Kangaroo Mother Care (KMC)
• Process of skin-to-skin care:
Considered culturally inappropriate as skin-to-skin contact is
involved between mother/father and child. Personal space is not
available for mother.
• Misconception amongst healthcare
professionals: May not be convinced of efficacy and benefits
of KMC.
• Role of father and other relatives:
Generally there is a misconception that giving skin-to-skin care
is the role of mother as she is the one breastfeeding. Fathers
and relatives are reluctant to provide Kangaroo care, which puts
the burden on the mother. Mother is given duty of household
chores preventing her from practising KMC.
• Considered as burden over staff:
Involves obtaining parents’ consent, feeding, teaching correct
method and follow-up. It is considered extra work for staff
which devoid of benefit for them
• Dilemma of policymakers: In a
majority of healthcare facilities, KMC is taken for granted as
part of routine care and no policies are available for its
implementation. Adequate space and basic facilities, which are
helpful for kangaroo position, are not provided or maintained
well.
|
There is enough evidence available now to show the
steps that can increase the implementation of KMC. Most of this evidence
is available from investigators outside India. From the evidence that is
available, one can draw the conclusion that the Indian effort towards
KMC care is not focused, and disorganized at best. Instead of training a
large number of people resulting in the expenditure of man-hours and
money; it might be more efficient and useful to train key opinion
leaders and interested faculty in areas where care is needed most.
Models of Implementation Across the World
The first qualitative study on the implementation of
KMC was conducted in South Africa in two hospitals in 1999-2000 to
identify important issues by interviews and direct observations [11,16].
Since 2000, regular KMC training workshops were held at the Kalafong
Hospital in Pretoria, which were evaluated by means of a questionnaire
asking about participants’ experiences of enabling factors and barriers
in currently practicing KMC or in implementing KMC in future [17].
Between 1994 and 2004, 44 teams in 25 developing
countries were trained in KMC in Bogota, Colombia; however, not all the
teams were successful in initiating their own programs and not all
replicated the validated model. A study was conducted in which
open-ended questionnaires were sent by e-mail to the coordinators of
functioning KMC programs in 15 countries, and 15 site visits were made
to institutes that reported problems in starting programs. They
concluded that active surveillance for an appropriate identification of
obstacles usually indicated the appropriate solution [18].
In a similar study conducted in India [19], the
barriers of KMC were categorized into six categories (knowledge,
mother-related, environmental, family-related, positional, and
infant-related barriers). One of the most important barriers of KMC was
lack of family members’ cooperation leading to inadequate time left for
the mother to stay by her infant constantly, as she does other household
activities and, consequently, spend the time to rest [19].
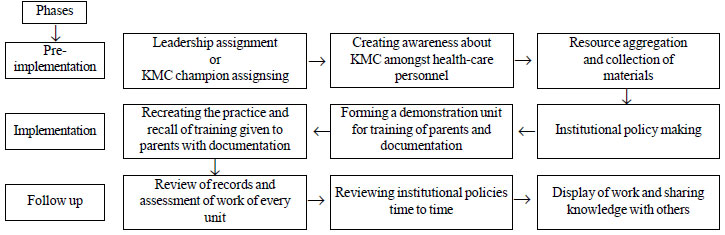
Proposed Model
Any regions, such as state or district or even a
healthcare organization, that wants to implement or propagate KMC can
structure its implementation plan as given below (Fig. 1).
It is derived from successful published experiences of implementation.
 |
|
Fig. 1 Stepwise approach for
implementation of Kangaroo mother care.
|
Our model for implementation of KMC is based on the
model developed from the studies conducted in South Africa. The steps
are, (i) Pre-implementation phase, (ii) Implementation and
(iii) Follow-up. This model for implementation is applicable for
institutes willing to adopt the concept of KMC for the benefit of
newborn babies.
First Phase: Pre-implementation
Leadership or KMC Champion: This is an
important concept that needs to be present in an effort to ensure KMC
implementation. For effective implementation of KMC on large scale, team
work is required and for that champions are allotted. The champions will
ensure that the effort is on track and should be able to address
obstacles in its implementation. The champions will have a leader for
keeping check over activities who will be able to convince the hierarchy
to allocate resources (personnel and budgetary allocation) for the KMC
program. It would be beneficial if the champions and leaders are experts
in KMC but it is not essential.
Creating Awareness about KMC: Healthcare
personnel need to be trained in both the need and the method of kangaroo
care. Multiple trainings to be carried out to ensure that challenges
towards the implementation of KMC that may arise can be dealt with. A
shoot and scoot kind of training approach will not help create
awareness.
Resource aggregation: This is the next part of
the program. This includes health personnel and educational material
such as videos, posters, papers, magazines, lectures, etc for purpose of
demonstration. In addition, materials required for implementation of KMC
(binders, caps etc.) need to be available and the administrative
processes with respect to the same needs to be in effect well in
advance.
Second Phase: Implementation
Policymaking: The center or institute should
formulate a policy regarding the implementation of KMC, taking the team
into confidence. The written policy with documents should be
user-friendly to health care workers involved and should be easily
applicable and accessible. Posters and magazines summarizing policy of
the institute should be displayed in the center, such that people are
aware of KMC, along with its benefits and implementation method.
Demonstration unit: This is the core of this
program. Preferably, a video recording along with good narration in
vernacular language and in English. Steps starting from room
temperature, to preparing of parents via counseling about KMC by
physician and/or nurse should be included. Mother preparation with
required clothes and other instructions should be clearly addressed.
Neonate preparation in terms of positioning, simultaneous monitoring of
vitals and all other required steps also need to be clearly
demonstrated. To enhance learning among healthcare providers, the
demonstration by the providers on parents (with prior consent), to
acclimatize them and revise all that’s learned should be done. Separate
workbooks can be given to all healthcare workers containing literature
and details about KMC showing benefits and pictorial representations of
KMC. Parents should be able to visit it, replicate what they have
learned on return and teach other parents. The first National conference
on Kangaroo Mother Care in India held in 2017 February had a
demonstration visit to Nalgonda SNCU for the excellent Kangaroo care
provided, which is a template that can be replicated across.
Recreating the Practice: After 2-4 weeks of
demonstration, health care providers who participated are gathered and
asked to demonstrate what they had learned and demonstrate it live on
babies. Accordingly, the score is provided. The practical demonstration
should be assessed frequently and amendments have done if required.
Third Phase: Follow-up
Review of records: the In-charge sister and
champions should make sure duration of KMC and other details should be
included in nursing records. Clinical review should be carried out every
monthly to track the usage of KMC. This essentially tracks the
improvement in KMC indicators over a period of time and discussion as to
what may have contributed to the change. The KMC champion leads the
review, but it may be a better idea if it is carried out by different
team members every time. Clinical review forms cornerstone for
successful implementation of KMC program as it helps to change viewpoint
of health care providers towards KMC implementation [20].
Assessment by unit in-charge:
Designated person to conduct timely assessment meets and makes sure
assigned work is completed and reviewed and a result if prepared.
In-charge also keeps quality of work by staff in check, and keeps
correcting and assessing them.
Reviewing policy: After audit information
gathered is applied to the current functioning of the system and based
on those; policies are reformed to improve the implementation of KMC.
Policies need to be updated from time to time to address issues that may
be the impeding duration of KMC.
Display of work and sharing knowledge:
This can be done by dissemination of program results, whether helpful or
not. This may be in the form of scientific articles or conference
presentations, as well by informing KMC champions in other institutions.
Active participation by other family members will help overcome the
hindrance created by maternal issues such as lack of proper maternal
surroundings and availability of her time [21]. Active participation of
mothers and their family members in the KMC process should be
appreciated in the form of certification and recognition in front of
other parents to motivate and boost their confidence in the process
The approach of training healthcare workers via
a teach the trainer model and expecting the healthcare system to change
will not work at all and needs to be abandoned in favor of an
implementation based program with a feedback to the implementing team.
The Road Ahead
While we delineate the model for implementation of
KMC, it needs to be studied during implementation and it may or may not
work in different settings. Any organization, planning to ramp up KMC
practices needs to audit and publish its practices. At this point of
time, three funded studies that are ongoing with the aim of increasing
the implementation of KMC in Haryana, Lucknow and Bengaluru [21-23].
Their results may not be replicable at all places. While the benefits of
KMC are proven for stable preterm, there is increasing evidence that it
may be even more useful for unstable preterm [24]. We also await the
results of an ongoing clinical trial in India that looks at KMC
beginning at birth [25]. The authors do feel that there is a need to
develop local strategies to enhance usage of KMC.
Though benefits of KMC are evident in reducing the
neonatal mortality rate, it alone is not sufficient for improving
mortality rate in low birth weight babies. A multidisciplinary approach
including good KMC, proper breastfeeding practices, handwashing and
hygiene maintenance, timely intervention for complications and regular
follow up in high risk clinic are needed by a competent team and
co-operative parents to improve overall neonatal mortality rate.
1. Conde Agudelo A, DíazRossello JL. Kangaroo mother
care to reduce morbidity and mortality in low birthweight infants.
Cochrane Database Syst Rev. 2016;20:5-36.
2. Lawn JE, Mwansa-Kambafwile J, Horta BL, Barros FC,
Cousens S. ‘Kangaroo mother care’ to prevent neonatal deaths due to
preterm birth complications. Int J Epidemiol. 2010;39:144-54.
3. Beck S, Wojdyla D, Say L, Betran AP, Merialdi M,
Requejo JH, et al. The worldwide incidence of preterm birth: A
systematic review of maternal mortality and morbidity. Bull World Health
Organ. 2010;88:31-8.
4. Lawn JE, Blencowe H, Oza S, You D, Lee AC, Waiswa
P, et al. Every newborn: Progress, priorities, and potential
beyond survival. Lancet. 2014;384:189-205.
5. Doddabasappa PN, Mahantshetti NS, Kamate M, Adarsh
E. Effect of Kangaroo mother care on neurodevelopmental outcome of low
birth weight babies: A one-year randomized control trial. Int J Contemp
Pediatr. 2018;5:508.
6. Charpak N, Tessier R, Ruiz JG, Hernandez JT, Uriza
F, Villegas J, et al. Twenty-year follow-up of Kangaroo mother
care versus traditional care. Pediatrics. 2017;139:e20162063.
7. Deorari A. Kangaroo Mother Care Initiative (KMCI).
Kangaroo Mother Care Initiative - Past Events. 2004. Available from:
http://www.kmcindia.org/healthcare/past_events.html. Accessed
February 26, 2019.
8. Vani S. About Us – Kangaroo Mother Care
Foundation. KMC foundation and KMC India conference. Available from:
https://kmcfoundationindia.org/index.php/about-us. Accessed February
17, 2019.
9. Soni A, Amin A, Patel DV, Fahey N, Shah N, Phatak
AG, et al. The presence of physician champions improved Kangaroo
mother care in rural Western India. Acta Paediatr. 2016;105:e390-395.
10. Nimbalkar S, Patel H, Dongara A, Patel DV, Bansal
S. Usage of EMBRACETM in Gujarat, India: Survey of pediatricians. Adv
Prev Med. 2014;415301.
11. Bergh A-M. Implementation-workbook-for-KMC.
Implementation workbook for Kangaroo mother care. Pretoria: Medical
Research Council Research Unit for Maternal and Infant Health Care
Strategies. 2002. p. 6-7.
12. Beiranvand S, Valizadeh F, Hosseinabadi R,
Pournia Y. The effects of skin-to-skin contact on temperature and
breastfeeding successfulness in full-term newborns after cesarean
delivery. Int J Pediatr. 2014;846486.
13. Cattaneo A, Amani A, Charpak N, De Leon-Mendoza
S, Moxon S, Nimbalkar S, et al. Report on an international
workshop on Kangaroo mother care: lessons learned and a vision for the
future. BMC Pregnancy Childbirth. 2018;18:170.
14. Seidman G, Unnikrishnan S, Kenny E, Myslinski S,
Cairns-Smith S, Mulligan B, et al. Barriers and enablers of
kangaroo mother care practice: a systematic review. PLoS One.
2015;10:e0125643.
15. Chan GJ, Labar AS, Wall S, Atun R. Kangaroo
mother care: A systematic review of barriers and enablers. Bull World
Health Organ. 2016;94:130-41J.
16. Bergh AM, Pattinson RC. Development of a
conceptual tool for the implementation of kangaroo mother care. Acta
Paediatr. 2003;92:709-14.
17. Bergh A-M, Arsalo I, Malan AF, Patrick M,
Pattinson RC, Phillips N. Measuring implementation progress in Kangaroo
mother care. Acta Paediatr. 2005;94:1102-8.
18. Pattinson RC, Arsalo I, Bergh A-M, Malan AF,
Patrick M, Phillips N. Implementation of Kangaroo mother care: a
randomized trial of two outreach strategies. Acta Paediatr.
2005;94:924-7.
19. Parikh S, Banker D, Shah U, Bala D. Barriers in
implementing community based kangaroo mother care in low income
community. Available from: http://paper.
researchbib.com/view/paper/3564. Accessed February 16, 2019
20. Joshi M, Sahoo T, Thukral A, Joshi P, Sethi A,
Agarwal R. Improving duration of Kangaroo mother care in a tertiary-care
neonatal unit: A quality improvement initiative. Indian Pediatr.
2018;55:744-7.
21. Clinical Trial Registry of India. Implementation
research in India (Karnataka state) towards accelerating scale-up of
Kangaroo Mother Care (KMC). 2017. Available from:
http://www.ctri.nic.in/Clinicaltrials/pdf_generate.php. Accessed
February 16, 2019.
22. ICH GCP - Clinical Trials Registry. Kangaroo
Mother Care Implementation Research for Accelerating Scale-up. Available
from: https://ichgcp.net/clinical-trials-registry/NCT03098069.
Accessed February 16, 2019.
23. Kumar A, Kumar V. ISRCTN - ISRCTN12286667:
Kangaroo Mother Care implementation research for accelerating scale-up
in Uttar Pradesh, India. Available from: https://www.isrctn.com/ISRCTN12286667.
Accessed February 16, 2019.
24. Chi Luong K, Long Nguyen T, Huynh Thi DH, Carrara
HP, Bergman NJ. Newly born low birthweight infants stabilise better in
skin-to-skin contact than when separated from their mothers: A
randomised controlled trial. Acta Paediatr. 2016;105:381-90.
25. Clinical Trials Registry of India. A
multi-country randomized clinical trial to evaluate the impact of
continuous KMC initiated immediately after birth compared to KMC
initiated after stabilization in newborns with birth weight 1.0 to less
than 1.8 kg on their survival in low-resource settings. Available from:
http://www.ctri.nic.in/Clinicaltrials/pmaindet2.php? trialid=21832.
Accessed February 26, 2019.


