|
|
|
Indian Pediatr 2018;55:757-760 |
 |
Improving the
Breastfeeding Practices in Healthy Neonates During Hospital Stay
Using Quality Improvement Methodology
|
|
Seema Sharma1,
Chanderdeep Sharma2
and Dinesh Kumar3
From 1Departments of Pediatrics, 2Obstetrics
and Gynaecology and 3Community Medicine, Dr Rajendra Prasad
Govt. Medical College, Himachal Pradesh, India.
Correspondence to: Dr Seema Sharma, House no 23,
Block-B,Type-V, DR RPGMCH, Kangra at Tanda,
Himachal Pradesh, India.
Email: dr.seema73.ss@gmail.com
Received: September 26, 2017;
Initial review: November 15, 2017;
Accepted: May 16, 2018.
|
Objective: To demonstrate the applications of the
principles of Quality Improvement (QI) in a tertiary-care centre
with the aim to improve the breastfeeding practices during hospital
stay.
Methods: An operational team was formulated to
identify the reasons for low proportion of exclusive breast feeding
(EBF) in healthy neonates. Reason specific solutions were proposed,
discussed, prioritized and tested using Plan-Do-Study-Act Cycle (PDSA
Cycle). Strategies included clear departmental policy plan and creation
of Breastfeeding support package (BFSP). PDSA cycles were tested and
implemented over 6 weeks period and its sustainability was measured
monthly for five months duration.
Results: After implementation of PDSA cycles,
the proportion of neonates receiving early breastfeeding within one
hour of birth increased from 55% to 95%, and the proportion of neonates
on EBF during hospital stay increased from 72% to 98%.
Conclusion: Quality Improvement principles are
feasible and effective to improve breastfeeding practices in the
hospital setting.
Keywords: Breastmilk, Baby friendly hospital, Exclusive
breastfeeding, Intervention.
|
|
Breastmilk is safe, available, affordable and one
of the most effective ways to ensure child health in developing
countries [1,2]. According to UNICEF, only 39 % of infants 0-5 month-old
in the developing world are exclusively breastfed (EBF). About 1.45
million lives are lost due to suboptimal/breastfeeding in developing
countries per year [3,4] . NFHS 4 data for 15 states from India shows
rise in institutional deliveries to 82.2%, with initiation of early
breastfeeding stagnant at 47.7%, and EBF values of 40% for the first six
months of life. This study aimed to improve the breastfeeding practices
during hospital stay, as hospital-based practices affect the duration
and exclusivity of breastfeeding throughout the first year of life. The
two main objectives were to increase the proportion of neonates
receiving early BF within one hour of birth from 55% to 90% and neonates
on EBF at the time of discharge from the hospital from 72% to 90%, over
a period of six months using principles of Quality improvement.
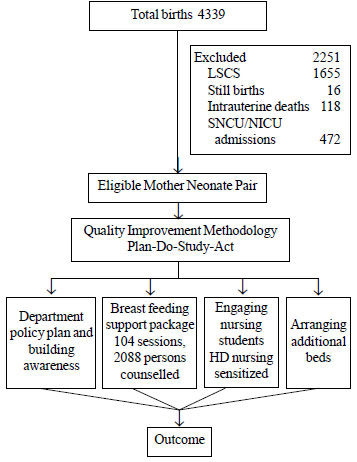
Methods
Mother-newborn pairs who were healthy and delivered
vaginally were included. Newborns delivered by lower segment caesarean
section, critically sick neonates, preterm neonates not on
breastfeeding/expressed breast milk, neonates of retro-positive mothers
who declined breastfeeding, and neonates having major congenital
malformations requiring surgical intervention were excluded (Fig.
1).
 |
|
Fig. 1 Study flow chart.
|
A team consisting of faculty members from departments
of Pediatrics, Obstetrics and Community Medicine; health educator; a
nutritional counselor; the sister in-charge of the labor room, and a
staff nurse from postnatal ward was constituted to evaluate the reasons
for Non-exclusive breastfeeding (NEBF) and to plan the strategy for the
promotion of optional breastfeeding practices. A baseline survey was
conducted by the Nutritional counselor for three days/week from 10:00 to
12:00 Hr and 14:00 to 16:00 Hr every day in December 2016, to know the
prevailing breastfeeding practices. It highlighted poor adherence to
standard guidelines, inappropriate provision and promotion of infant
formula. Focussed Group discussions (FGDs) were followed by fish bone
analysis, which revealed that the reasons for NEBF were related to
policy, people, place and processes. Lack of knowledge, sensitization of
health care providers and lack of support for the mothers were few of
the vital reasons limiting the BFP (Web Fig. 1).
Suggested solutions were prioritized and each
proposed solution was considered as a change idea and was tested on five
mothers for one day in order to adopt or adapt the proposed solution.
There were four change ideas which were applied weekly for the period of
six weeks. The data was collected after each Plan-Do-Study-Act (PDSA)
cycle for 3 days/week for six weeks initially to see the feasibility. To
assess the sustainability of the Quality-improvement (QI) practices,
subsequent data collection was done monthly for a period of five months
in a manner similar to the baseline assessment. The team met weekly for
six weeks, followed by monthly meetings for five months. The change
ideas were implemented as PDSA Cycles in accordance with QI principles.
PDSA Cycle I: Department policy plan and building
awareness amongst health care providers: A policy plan regarding
breastfeeding practices was circulated amongst all health care providers
with the emphasis on not prescribing formula feed unless clinically
indicated. To create awareness in healthcare providers, FGDs with
residents, in-charge sisters and nursing sister of labor room and sick
newborn care unit (SNCU) were carried out. A poster was displayed in the
labor room for dissemination of the information.
PDSA II: Breastfeeding support package:
The data showed that merely building awareness and making policy clear,
changes the pattern of breastfeeding practices; through, some resistance
from the mothers and their attendants was observed. During third week,
team came up with the idea of delivering a BFSP, the components are
depicted in Box I.
|
Box I Components of Breastfeeding
Support Package
• Counselling of the mothers and attendants
in the group of 15-20, on breastfeeding practices and its
benefits, in the labor room and postnatal ward using IYCF
(Infant and young child feeding) guidelines.
• One ear-marked SNCU nursing sister to be
posted in each shift in the labor room - NBCC (Newborn Care
Corner) to ensure early initiation of breast feeding.
• Additional support was provided by the
nursing staff in the postnatal ward to provide practical help to
the mothers.
|
PDSA III: Engaging nursing students: To deliver
BFSP to each and every mother, team decided to engage nursing students
present in all the shifts in the labor room and postnatal ward. Nursing
students were sensitized under the supervision of health educator and
counselor. Finally, nursing students started providing BFSP throughout
their posting.
PDSA IV: Arranging additional beds: Although data
started showing improvement in the BFP, team realized that mothers are
shifted soon after delivery from labor room to postnatal ward, which was
making early initiation of BF difficult. Hence, to provide bedding-in
facility, the team arranged additional 10 beds for mothers outside the
labor room in the fourth week. The additional benefits were prolonged
observation of mothers for any complications after delivery and their
counselling on nutrition and family planning which was missed earlier.
The team members shared the results of interventions
and gave continuous feedback to staff and resident doctors involved in
clinical care.
Results
In the baseline survey, out of total 280 healthy
neonates, 154 (55%) had received early breastfeeding. Out of remaining
126 (45%), 78 (28%) had received non-breast milk supplements and 48
(17%) received nothing. During hospital stay, 78 (28%) of the healthy
neonates were not on EBF. These neonates were receiving either infant
formula feed or mixed feeds (breastfeeding along with formula feed).
Amongst total 280 mothers, 154 (55%) were primigravida. About one third
of multiparous mothers had unsatisfactory experience of breastfeeding
due to poor positioning and poor attachment.
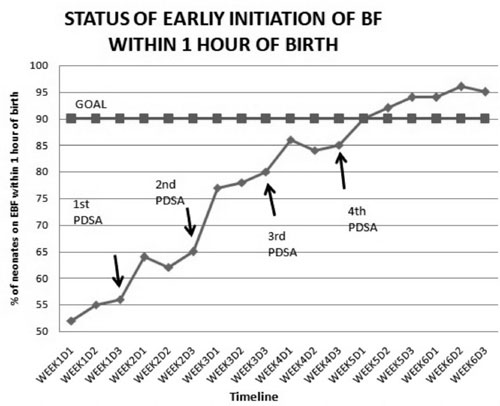
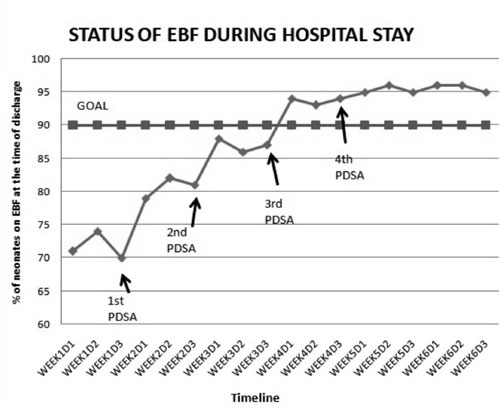
After four PDSA cycles, the proportion of neonates
receiving early breastfeeding within one hour of birth increased from
55% to 95% and the proportion of neonates on EBF during hospital stay
increased from 72% to 98% (Fig. 2 a and b).
 |
| (a) |
 |
| (b) |
|
Fig. 2 (a) Status of early initiation
of breastfeeding within one hour of birth; (b) Status of
exclusive breastfeeding during hospital stay.
|
The assessment for sustainability for five months
revealed that trend of improved BFP remained above 95%. To ensure smooth
running of system, healthcare providers were oriented on optional
breastfeeding practices at the time of their joining.
Discussion
Low- and middle-income countries lose more than $70
billion annually due to low rates of breastfeeding. Universalization of
breastfeeding in India may reduce 1,56,000 under-5 deaths, 39,00,000
episodes of diarrhea, 34,36,560 episodes of pneumonia and 7,000 deaths
due to breast cancer annually [1,2]. Our root cause analysis showed
widespread use of NEBF to be due to poor antenatal care, and lack of
information on optimal infant feeding, especially EBF, given by health
workers at health institutions. This study revealed that lack of early
initiation of BF, lack of bedding-in facility and not giving EBF during
their last pregnancy was associated with NEBF. Inappropriate provision
and promotion of infant formula were common, despite evidence that such
practices reduce BF success. These findings are in accordance with the
available literature [5-7]. In our study, rates of early initiation of
BF and EBF increased significantly during hospital stay. It showed
sustainability of 95% even after 6 months of implementation. These
results show impact similar to the previous work done to improve EBF
rates using QI principles [8-12].
Our study showed processes and system changes
resulted into improvement in BFP. Important reductions in morbidity and
health care costs with a positive public impact are possible if our
method of QI is widely disseminated. A study on impact of optional
breastfeeding practices BFP during hospital stay on continuation of EBF
upto 6 months of age could have strengthened our study results.
The present study suggests that QI principles are
feasible and lead to improved rates of BFP during hospital stay. This is
a single centre QI initiative done with the involvement of existing
caregivers and executed without any external funding in the form of
manpower or financial assistance, which suggests the importance of
simple and feasible QI principles using team approach. Formation of a
breastfeeding support group is the next step to sustain these practices.
This QI initiative has helped our institute to improve breastfeeding
practices by transforming maternity practices to better support mothers
who choose to breastfeed. Such efforts, could affect both initiation and
duration of breastfeeding, with substantial, lasting benefits for
maternal and child health.
Acknowledgements: The authors acknowledge
the support of USAID Team consisting of Dr Nigel, Mr Praveen and Dr
Anjali for introducing them to the concept of quality improvement and
hand holding during this QI project.
Contributors: SS: has conceptualized the
concept; SS,CD,DK: were involved into collection of data and its
analysis. All authors approved the final manuscript.
Funding: None; Competing Interest: None
stated.
|
What This Study Adds?
• Quality Improvement principles are feasible and effective
to improve exclusive breast feeding practices in the
hospital-setting.
|
References
1. Essential Nutrition Actions: Improving Maternal,
Newborn, Infant and Young Child Health and Nutrition. Geneva: World
Health Organization; 2013. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK258736/. Accessed March 18,
2018.
2. Planning Guide for National Implementation of the
Global strategy for Infant and Young Child Feeding. World Health
Organization; 2013. Available from:
https://www.int/nutrition/publications/infant feeding/9789241595193/en/.
Accessed March 18, 2018.
3. Breastfeeding: Impact on Child Survival and Global
Situation. New York: UNICEF; 2014. Available from:
https://www.unicef.org/nutrition/index_24824.html. Accessed March
18, 2018.
4. Lauer JA, Betran AP, Barros AJ, Md O. Deaths and
years of life lost due to suboptimal breastfeeding among children in the
developing world: A global ecological risk assessment. Public Health
Nutr. 2005;9:673-85.
5. Agho KE, Dibley MJ, Odiase JI, Ogbonmwan SM.
Determinants of exclusive breastfeeding in Nigeria. BMC Pregnancy
Childbirth. 2011;11:2.
6. Woldie TG, Kassa AW, Edris M. Assessment of
exclusive breastfeeding practice and associated factors in Mecha
District, North West Ethiopia. Sci J Public Health. 2014;2:330-6.
7. The State of the World’s Children. UNICEF, 2000.
Available from: www.unicef.org/sowc00/stat4htm. Accessed March
18, 2018.
8. Mercier CE, Barry SE, Paul K, Delaney TV, Horbar
JD, Richard C, et al. Improving newborn preventive services at
the birth hospitalization: A collaborative, hospital-based
quality-improvement project. Pediatrics. 2007;120:481-8.
9. Kuzma-O’Reilly B, Duenas ML, Greecher C, Kimberlin
L, Mujsce D, Walker DJ. Evaluation, development, and implementation of
potentially better practices in neonatal intensive care nutrition.
Pediatrics. 2003;111:e461-70.
10. Bloom BT, Mulligan J, Arnold C, Ellis S, Moffitt
S, Rivera A, et al. Improving growth of very low birth weight
infants in the first 28 days. Pediatrics. 2003;112:8-14.
11. Merewood A, Philipp BL, Chawla N, Cimo S. The
baby-friendly hospital initiative increases breastfeeding rates in a US
neonatal intensive care unit. J Hum Lactation. 2003;19:166-71.
12. Sethi A, Joshi M, Thukral A, Dalal JS, Deorari
AK. A quality improvement initiative: Improving exclusive breastfeeding
rates of preterm neonates. Indian J Pediatr. 2017;84:322-5.
|
|
|
 |
|
