A
chalasia cardia is rare in children, with a
reported incidence of 0.11per lakh. Less than 5% of patients with
symptomatic achalasia present below 15 years of age and of these less
than 1 % are infants [1]. First case in an infant was reported by King
in 1953 [2]. It is characterized by failure of lower esophageal
sphincter (LES) to relax in response to swallowing. It is often
misdiagnosed as gastroesophageal reflux disease (GERD), which may lead
to significant delay in diagnosis.
Case-report
Case 1: A nine-month-old boy presented with
recurrent non-bilious vomiting containing undigested feeds, repeated
chest infections and failure to thrive (weight 4.5 kg, z score <–3
SD, height 70 cm). He had received treatment for
GERD, but without any relief. Routine investigations revealed
leucocytosis (62,900/mm3)
with lymphocytosis and positive procalcitonin. Cytomegalo-virus (CMV)
IgM and PCR were positive. He was started on intravenous Ganciclovir.
Upper gastro-intestinal (UGI) endoscopy showed dilated esophagus. Barium
swallow showed a dilated thoracic esophagus and narrowing at GE junction
(Fig. 1) suggestive of achalasia cardia. After
optimization, he underwent Heller’s cardiomyotomy with Dor’s anterior
fundoplication. At 6 months follow-up, baby had significant weight gain
(weight 9 kg).
 |
|
Fig. 1 Upper GI contrast study in
case 1, showing bird-beak sign.
|
Case 2: This 18-month-old boy presented with
complaints of recurrent lower respiratory tract infections and vomiting
after feeds since the age of 7 months. He weighed 7.3 kg (z score <–2
SD, and height 81.2 cm). Routine investigations revealed leucocytosis
(22,000/mm3) and X-ray
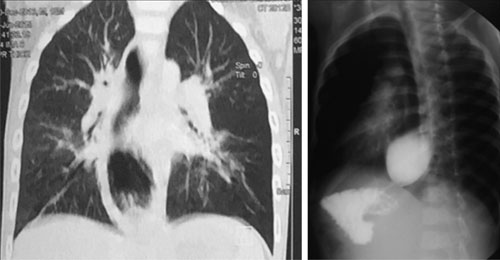
chest showed bilateral lung infiltrates. Contrast CT scan chest done
outside revealed a dilated thoracic esophagus. Contrast swallow study
showed characteristic ‘bird beak’ sign which confirmed the diagnosis of
achalasia cardia (Fig. 2) for which he underwent surgery.
Six months post-operatively he had achieved weight of 10 kg.
 |
|
Fig. 2 CECT chest showing dilated thoracic
esophagus and upper GI contrast study showing megaesophagus in
case 2.
|
Case 3: This 12-month-old presented with
complaints of recurrent vomiting of uncurdled milk, since the age of 2
months. He weighed 6.5 kg (at–3 SD) and height was 73.4 cm. Contrast
swallow study showed classical ‘bird beak’ sign confirming the diagnosis
of achalasia cardia. He underwent Heller’s cardiomyotomy and had
significant symptomatic relief post-operatively.
Discussion
Achalasia cardia is a neuromuscular disorder
characterized by degenerative changes of the myenteric plexus leading to
selective loss of inhibitory nerve endings. This characteristically
leads to failure of the coordinated muscle relaxation mechanism of LES
after a peristaltic contraction of the esophageal body, stimulated by
deglutition. Achalasia cardia can be classified as primary or secondary.
Primary achalasia is a part of Allgrove and Alport syndrome, and is also
seen in Down syndrome [3]. An association with some viral infections
(Epstein Barr, herpes simplex and varicella zoster) has been described
[3].
The most common characteristic feature of infantile
achalasia is vomiting of uncurdled milk, which is also seen in
regurgitation occurring commonly with faulty-feeding or over-feeding in
infants and hence, it is usually missed initially. This kind of vomiting
is also seen in infants with GERD. Frequently occurring complications of
GERD such as aspiration pneumonia, esophagitis, midline chest pain,
refusal to feed, failure to gain weight and anemia are also seen in
achalasia cardia [4]. To rule out other esophageal disorders, UGI
endoscopy followed by UGI contrast study is done. Manometry is the
definitive investigation for diagnosis of achalasia cardia, but due to
technical difficulties it is rarely done in infants [5].
Medical management of achalasia includes oral drugs
like nitrates, calcium channel blockers and 5-phosphodiesterase
inhibitors [5]. Pharmacological therapies provide temporary relief of
symptoms and have not been recommended in infants [5]. Endoscopic
injection of botulinum toxin has been used in adults but not preferred
in infants [6]. Endoscopic balloon dilatation has been used in pediatric
patients with achalasia but is not a preferred option due to associated
complications such as perforation and short lasting effect [3]. Another
non-surgical treatment modality described recently in adults and older
children is per-oral endoscopic myotomy (POEM). It is a technically
challenging procedure with 18% failure rate and high incidence of
esophagitis (42%), esophageal perforation and GERD [6].
Heller’s myotomy with anti-reflux procedure, is the
gold standard for management of achalasia cardia. Symptomatic relief
post-surgery is reported in 95% cases [6]. Although achalasia is rare in
infancy yet it should be kept in mind if there is persistent
regurgitation of feeds with failure to gain weight or repeated chest
infections. It can be diagnosed easily by upper GI contrast study.
Contributors: RB: designed the paper and prepared
the manuscript; AP: helped with preparation of manuscript, overall co-ordinator
and guide and will act as guarantor for the paper; VK: helped in
reviewing the literature and investigating the cases; NW: involved with
diagnosis and medical management of the cases.
Funding: None; Competing interest: None
stated.
References
1. Chatterjee S, Gajbhiye V, De A, Nath S, Ghosh D,
Das SK. Achalasia cardia in infants: Report of two cases. Journal of
Indian Medical Association. 2012;44:1-5.
2. Sarangapani A, Vijayaraghavan S, Shanmuganathan S,
Rajanikanth S. Achalasia cardia in infant. Sri Lanka J Infant Health.
2010;40:74-5.
3. Franklin AL, Petrosyn M, Kane TD. Infanthood
achalasia: a comprehensive review of disease, diagnosis and therapeutic
management. World J Gastrointest Endosc. 2014;6:105-11.
4. Rai GS, Sarawagi R, Sharma S, Apte A. An infant
with nasal regurgitation since birth and failure to thrive. J Clin Diagn
Res. 2015;9:3.
5. Dughera L, Chiaverina M, Cacciotella L, Fabio C.
Management of achalasia. Clin Exp Gastroenterol. 2011;4:33-41.
6. Patti MG, Fischella PM. Controversies in management of Achalasia.
J Gastrointest Surg. 2014;18:1705-9.


