|
|
|
Indian Pediatr 2013;50: 887-888 |
 |
Disulfiram Poisoning Causing Acute
Encephalopathy
|
|
Vykuntaraju KN and *Arvinda Hanumanthapura Ramalingaiah
Division of Pediatric Neurology, Indira Gandhi
Institute of Child Health, Bangalore and *Department of Neuro-radiology,
National Institute of Mental Health and Neurosciences (NIMHANS),
Bangalore, Karnataka, India.
Email: [email protected]
|
Disulfiram is used for the treatment of alcoholism, exerts
its action when taken concomitantly with alcohol. The
typical reaction is self-limited, with headache, flushing,
dizziness, nausea, blurred vision, tremor and dyspnea [1].
When not associated with alcohol ingestion, its effects are
scarce at usual daily doses. Acute intoxication at doses
higher than 500 mg/d, may result in severe collateral
effects, and can be lethal at doses between 10-30g/d [2].
The presence of this drug in the home makes it a potential
agent for accidental poisoning. We report an unusual case of
disulfiram poisoning.
A two-year-old healthy boy presented with
lethargy, drowsiness and unresponsiveness of one day
duration. No history of fever, trauma and parents denied any
intoxication. His development was appropriate for age. There
was no significant family history. Later the subject
developed convulsions, persistent encephalopathy and
dystonia. On examination, his anthropometry was normal. He
had acidotic breathing with hypotension (blood
pressure-60/40mm). His Glasgow coma scale was 6/15. The
pupils and fudus were normal. Dystonia was present. There
were no signs of meningeal irritations. Differential
diagnosis of metabolic encephalopathy, encephalitis and
intoxication were considered.
Hematological and biochemical workup
including serum electrolytes, serum lactate and ammonia
levels were normal. Arterial blood gas was suggestive
of severe metabolic acidosis (pH-7.02, PO 2-75,
PCO2-12, HCO3-6
BE- -16). Cerebrospinal fluid examination was normal.
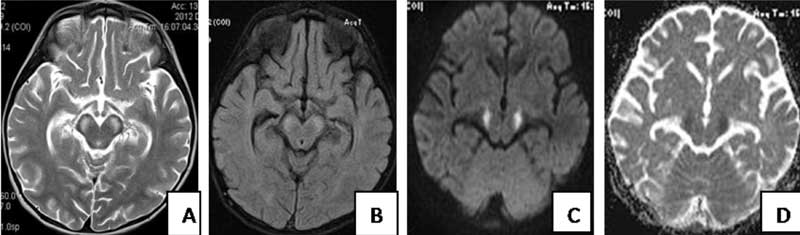
MRI of brain showed swollen and symmetrical hyperintense
signal changes involving the globus pallidus and substantia
nigra. Additionally both the structures are showing
restricted diffusion on DWI images (Fig. 1).
Tandem mass spectroscopy (TMS) and gas chromatography and
mass spectroscopy (GC/MS) of urine were found to be normal.
After 2 weeks the boy’s father reported that 8-10 of the
disulfiram tablets, that the grandfather was on, were
missing. The clinical findings, acidosis and MRI findings
were consistent with disulfiram poisoning. Treatment with
megavitamins was started but child had persistent
extra-pyramidal symptoms with minimal improvement in
sensorium after one month of consumption of disulfiram.
 |
|
Fig. 1 A,B,C and D
represents axial T2WI, FLAIR and axial DWI and ADC
maps taken at the level of crus cerebri
respectively. They show swollen and symmetrical
hyperintense signal changes involving the globus
pallidus and substantia nigra. Additionally
restricted diffusion is seen on DWI images.
|
The diagnosis of disulfiram poisoning is
difficult as it is rapidly cleared from the circulation; its
metabolites can be measured only by highly specialized
laboratory techniques, which are not readily available.
There is no specific antidote for disulfiram toxicity.
The exact mechanism of disulfiram
mediated encephalopathy is not known. However, disulfiram
metabolites diethyldithiocarbamate and carbon disulfide have
been shown to inhibit the activity of the enzyme dopamine-a-hydroxylase
leading to the accumulation of dopamine, producing a
relative deficiency of adrenaline and noradrenaline in the
area of the basal ganglia. Dopamine-mediated cellular injury
may be related to its ability to induce excitatoxic effects
of glutamate; - calcium mediated cell death, and impairs the
cellular ability to eliminate free oxygen radicals [3].
The possible differential diagnosis of
Leigh’s Disease, Organic acidurias, and carbon monoxide
poisoning were considered but ruled out on history, clinical
features and MRI findings. We ruled out extrapontine
myelinolysis as his serum sodium levels were within normal.
Disulfiram poisoning should be suspected
in any child presenting with unknown encephalopathy with
convulsions, extra-pyramidal symptoms with basal ganglia
signal changes in MRI of brain in a previously normal child.
Acknowledgments: Dr Kavitha V and
Dr Arvind Kasaragod for their help in management of the
case.
References
1. Wright C, Moore RD. Disulfiram
treatment of alcoholism. Am J Med. 1990;88:647-55.
2. Petersen EN. The pharmacology and
toxicology of disulfiram and its metabolites. Acta Psychiatr
Scand Suppl. 1992;369:7-13.
3. Rothmann S, Olney J. Glutamate and the pathophysiology
of hypoxicischemia damage. Ann Neurol. 1986;19: 105-111.
|
|
|
 |
|
