Hemimegalencephaly is a rare congenital brain malformation involving
enlargement of only one cerebral hemisphere(1). Hemimegalencephaly is a
type of hamartomatous lesion(2) or migration disorder, but its etiology
remains unknown. Patients with the syndromic form of the disease have
underlying disorders, most of which are neuro-cutaneous syndromes. Those
with the isolated form of hemimegalencephaly have no such disorders.
Usually hemimegalencephaly is suspected due to a large head, early onset
of intractable seizures, hemiparesis, and/or skin lesions. We report a
case of infant with incidentally detected hemimegalence-phaly having
global developmental delay and microcephaly.
A 6 month old girl infant first born of non
consanguineous marriage, having global develop-mental delay (developmental
age 2-3 months), presented for the first time with atypical generalized
febrile convulsion (multiple). Perinatal history was uneventful.
Clinically she was well nourished on breast feeds. Head was dolicocephalic
with some sloping of forehead (head circumference 36 cm, microcephaly) all
sutures were fused, weight 6.5 kg and length 65 cm. She had no dysmorphism
or asymmetry of face and body. There were no neurocutaneous markers. In
the absence of perinatal adverse events and fused cranial sutures, primary
craniostenosis versus cerebral dysgenesis were considered as
differential diagnosis.
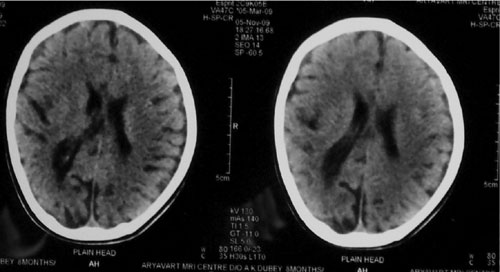
EEG showed multifocal epileptical abnormalities and CT
brain showed right sided hemimegalencephaly (Fig 1). She was
put on sodium valproate and stimulation therapy. On follow up till ten
months of age she had developmental age of 8-9 months. There was no
recurrence of seizures.
In hemimegalencephaly, heterotopic neurons are immature
and are of both neuronal and glial cell lineage(3). Glial proliferation
has also been reported to explain the increased volume of white matter(4).
It is generally suspected in patient with large head, intractable seizures
and hemiparesis, or its association with neurocutaneous syndromes. Our
patient had presented with microcephaly and atypical febrile convulsion
with global develop-mental delay but had no hemiparesis even on follow up.
Diagnosis is straightforward with neuroimaging, preferably MRI which can
grade and pick up migration disorder(5).
References
1. Flores-Sarnat L. Hemimegalencephaly. Part 1.
Genetic, clinical, and imaging aspects. J Child Neurol 2002; 17: 373-384.
2. Townsend JJ, Nielsen SL, Malamud N. Unilateral
megalencephaly. Hamartoma or neoplasm?. Neurology 1975; 25: 448-453.
3. Flores-Sarnat L, Sarnat HB, Davila-Gutierrez G,
Alvarez A. Hemimegalencephaly. Part 2. Neuropathology suggests a disorder
of cellular lineage. J Child Neurol 2003;18: 776-785.
4. Kato M, Mizuguchi M, Sakuta R, Takashima S.
Hypertrophy of the cerebral white matter in hemimegalencephaly Pediatr
Neurol 1996; 14: 335-338.
5. Battaglia D, Di Ricco C, Iuvone L, Acquafondata C,
Iannelli A, Lettori D, et al. Neuro-cognitive development and
epilepsy outcome in children with surgically treated hemimegalencephaly
Neuro-pediatrics 1999; 30: 307-313.