|
|
Lead Article Indian Pediatrics 2007; 44: 649-656 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Role of Dexamethasone and Oral Glycerol in Reducing Hearing and Neurological Sequelae in Children with Bacterial Meningitis |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Jhuma Sankar, P Singhi, A Bansal, P Ray and S Singhi From the Department of Pediatrics, Advanced Pediatric Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India. Correspondence to: Dr. Sunit Singhi, Professor of Pediatrics, Advanced Pediatric Center, PGIMER, Chandigarh 160 012, India. E-mail: drsinghi@glide.net.in Manuscript received: August 21, 2006; Initial review
completed: October 10, 2006;
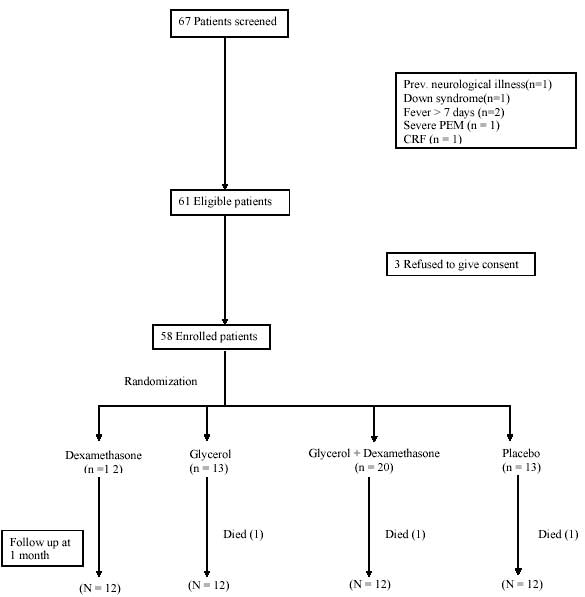
Hearing deficit is the most common complication of bacterial meningitis(1-3). Severe neurological sequelae such as quadriparesis, spasticity or mental retardation can also occur(4-7). It has been proposed that the prognosis of bacterial meningitis can be significantly improved with adjunctive treatment with dexamethasone or glycerol. Several trials suggest that dexamethasone might reduce auditory sequelae, especially those of Hib meningitis, but not fatality rate(8-10); other studies have found no benefit(11-13). A WHO expert committee in 1997 concluded "there is insufficient evidence to support recommendations for the routine use of steroids for all children with bacterial meningitis"(14). Glycerol was compared with dexamethasone in treatment of bacterial meningitis in a multicenter randomised controlled trial in Finland(15); oral glycerol prevented severe or profound bilateral hearing loss more efficiently than intravenous dexamethasone. Also glycerol compared favorably when all neurological abnormalities after 3-6 months of discharge were combined(15). The objective of this randomized 4-arm study was to examine efficacy of dexamethasone vs. oral glycerol or a combination of both, in reducing auditory and neurological sequelae of childhood bacterial meningitis. Subjects and Methods This was a prospective double blind placebo controlled randomized study conducted in the Pediatrics Services of a tertiary care teaching hospital in North India. Children diagnosed as acute bacterial meningitis admitted between June 2002 and September 2003 were enrolled. Institutional Ethics committee had approved the study. Informed written consent was obtained from the parents. Children (2 month-12 years) with acute onset of fever (<1 week duration) and signs of CNS involvement (such as irritability, lethargy, convulsion, neck stiffness etc) were included. A diagnosis of bacterial meningitis was accepted in presence of (i) positive CSF culture; (ii) positive blood culture; (iii) positive latex agglutination test; or (iv) suggestive CSF cytology and biochemical profile. Children with previously diagnosed neurological disability, those with ventriculoperitoneal shunt, severe malnutrition (weight for age <60%), immunosuppressed state, any chronic illness and those having sustained trauma were excluded. Children who had received more than one dose of intravenous antimicrobial therapy before diagnosis were also excluded. Data were collected on demographic profile, clinical presentation, CSF findings and hematological and biochemical profile of study subjects. Children were randomized to receive: 1. Glycerol (1.5 g/kg every 6 hourly) oral/ nasogastric tube + placebo (normal saline) intra-venous (IV). 2. Dexamethasone (0.15 mg/kg every 6 hourly) IV + placebo (carboxymethylcellulose solution 2%) oral / nasogastric tube. 3. Glycerol oral/ nasogastric tube + dexamethasone IV. 4. Placebo (carboxymethylcellulose solution 2%) oral / nasogastric tube + placebo (normal saline) IV. Ceftriaxone 100 mg/kg/day intravenously was administered to all patients once a day for a minimum of 7 days. A randomization list was prepared using simple random number table. Serially numbered sealed packets each containing drugs and placebo were prepared as per randomization and were kept readily available, 24 hours a day, for the doctor on duty. Neither the treating clinician nor the patients were aware of the nature of the drugs used. A person not directly involved with patient assignment, data collection and analysis prepared the packets. Randomization codes were broken after the initial analysis was done. Follow-up Examination The patients were examined thoroughly at least once daily during hospitalization and clinical details were noted. Computed tomography scan was done when clinically indicated. All survivors were assessed at the time of discharge from hospital and one month after discharge for neurological and hearing impairment. Neurological abnormalities were recorded as major or minor neurodeficits. Major deficits included blindness, quadriparesis, hemiparesis, severe psychomotor retardation, and hydrocephalus. Minor deficits included monoparesis, moderate psychomotor retardation and ataxia. Psychomotor retardation was assessed in a follow up clinic by Denver developmental scale II (DDST-II) by a physician not involved in the study. Fundoscopic examination and Visual Evoked Potential (VEP) were used to evaluate blindness. Hydrocephalus was evaluated by serial monitoring of occipitofrontal head circumference and computed tomography. Hearing was tested by either play audiometry (co-operative children >2.5 years) or by brainstem evoked auditory potential (BERA) (children <2.5 years) at 1 month after discharge. A hearing thres-hold level of 21-40 dB indicated mild, 41-60dB moderate, 61-80 dB moderately severe, 81-100dB severe, and >100 dB profound impairment. Statistical analysis: Descriptive statistics were calculated. Statistical analysis was performed with SPSS for Windows, version 10.0. Comparison of means was done by ANOVA or t-test and of categoric variables by Chi-square test. Results The study flow chart, recruitment and randomization are depicted in Fig 1. The clinical and laboratory characteristics of the subjects in the four groups are shown in Table I. Signs of raised ICP at admission were present in 37 (63.7%) patients. The mean blood pressure at admission was between the 50th and 95th centile in most children. The capillary filling time was between 2-3 seconds in all cases. The CSF leukocyte count was predominantly polymorphonuclear, and ranged from 10-2800 (mean ± SD 350 ± 548) mm3. Thirty-four (58%) patients had counts between 100 to 999 cells/ mm3. CSF glucose values <40 mg/dL were seen in 23 (39%) patients. CSF protein ranged from 20-140 mg/dL. Serum CRP ranged between 42-192 mg/dL. Fourteen (24%) patients had a total leukocyte count of >15000/mm3. A bacterial etiology could be established in 24 patients (Table I).
TABLE I Clinical and Laboratory Characteristics of 58 Study Patients
a Data expressed as mean ± SD. b Data in parenthesis are column percentage unless otherwise indicated. * P = 0.02 between placebo and glycerol groups; P = 0.03 between placebo and dexamethasone groups (CSF glucose). The ‘P’ value between the groups for other parameters was not statistically significant. Radio-imaging was obtained in 23 (39%) patients because of focal neurological deficits, repeated seizures or altered sensorium. Ten patients showed abnormalities, which included infarcts (one each in dexamethasone + glycerol and placebo + placebo group), hydrocephalus (one in each group except dexamethasone group), cerebral edema (one each in dexamethasone and glycerol group), meningeal enhancements (in placebo group) and large subdural effusion (both in placebo group). Forty-eight patients received ceftriaxone for 7 days. Ten patients received longer course of ceftriaxone and/or an additional antibiotic because of poor clinical response (n = 2), organism not sensitive to ceftriaxone (n = 4) and nosocomial infection (n = 2). Of the five patients with CSF positive for Staphylococcus aureus, three received vancomycin and two cloxacillin plus gentamicin. Three patients died; one in each group except dexamethasone group. Hospital stay was ≤ 7 days in 76% (n = 10) patients in glycerol group and 91% (n = 11) patients in dexamethasone group.Fifty-one (88%) children were afebrile by day 6; this was similar in all the 4 groups. The four groups did not show any difference with respect to recovery from other symptoms. Of the 10 patients with a GCS score <8, two were in placebo group; one of them died by day 4 and the other improved. Both the children were mechanically ventilated for a short duration. The sensorium returned to normal in all the other patients by day 6. Overall, 52 (95%) of 55 survivors had a GCS score >8 by day 6. Three cases of GI bleeding were reported, one each in dexa-methasone + glycerol, placebo and dexamethasone groups. Neurological and hearing sequelae Neurological sequelae were present at one month follow up in 7 (12 %) patients; in 3 patients in glycerol, 3 in dexamethasone+glycerol and 1 in placebo group (P = 0.29). Quadriplegia was seen in three patients (one patient each in glycerol, dexamethasone and placebo group). Severe psychomotor retardation was seen in 2 patients (one each in the glycerol and glycerol + dexamethasone groups). One had improved to mild psychomotor retardation at 6 months follow-up. Hydrocephalus was seen in two patients (one patient each in glycerol and glycerol + dexamethasone groups). Blindness was seen in two patients one each in glycerol and glycerol + dexa-methasone groups. Hemiparesis was seen in two patients after one month of discharge (one each in glycerol and placebo groups). Monoparesis was not seen in any subject. Moderate psychomotor retardation was seen in one patient in dexamethasone + glycerol group. He also had ataxia. Neurological sequelae were present at 6 months follow-up in 6 of seven children having sequelae at one-month follow-up. Audiologic assessment was performed using pure tone audiometry in 15 children and BERA in the remaining 40. Results are depicted in Table II. The abnormalities detected on BERA included increased latencies (I-III waves, & I-Vwaves) and decreased amplitude of wave V. Six children had bilateral hearing loss while 4 had left sided hearing loss ranging from mild to profound hearing impairment. The incidence of hearing impairment and its severity was not significantly different in the four groups (P = 0.68). TABLE II Hearing sequelae in the four groups
* Figures in parantheses indicate column percentages Discussion Hearing and neurological sequelae are common in children with bacterial meningitis (16-19). Our study showed no significant difference in the frequency of hearing sequelae either with the use of dexamethasone or glycerol. Similarly, there was no statistical difference in the neurological outcome with either dexamethasone or glycerol or both combined, in children with acute bacterial meningitis. This is in accordance with the studies that have found no clear advantage of the use of dexamethasone as an adjunctive therapy in reducing the hearing or neurological sequelae in children(11-13). The results of our study are in contrast with the Finnish study in which glycerol was shown to prevent severe hearing loss and also neurological sequelae(15). Glycerol, an osmotic diuretic, has been used in reducing intracranial pressure in various neurosurgical and neurological disorders (20-22) but its role in prevention of sequelae in bacterial meningitis is scarcely reported(15). It lowers ICP through the build-up of an osmotic gradient. Absence of beneficial effect of glycerol in our study could partly be explained by the rebound phenomenon leading to worsening of brain edema, which may occur if there is an increase in the glycerol concentration in the cerebrospinal fluid(23). Also a real difference might not have been detected because of the small sample size. Studies, mostly from developed countries, have advocated the use of dexamethasone as part of the initial regimen for management of bacterial meningitis as these randomized studies found a reduction in neurological sequelae with the use of dexamethasone(8-10,24-26). The benefits of dexamethasone treatment in children in reducing both hearing and neurological sequelae have been shown in various other studies even though the benefits have varied(26,27). In a study by Kanra, et al. the long term neurological outcome including hearing impairment was better in the dexamethasone treated patients(28). Bilateral hearing loss was not observed in the dexamethasone treated patients whereas 7.6% of non-dexamethasone patients had bilateral hearing impairment. Odio, et al. found the incidence of neurologic sequelae was less in patients receiving dexamethasone (14%, P= 0.007)(8). All the above studies were from developed countries and most of them were in favor of the use of dexamethasone as an adjunctive therapy in childhood bacterial meningitis except a few. However, studies from developing countries produced different results from those in developed countries(12). The Malawi trial has shown that use of dexamethasone did not improve overall outcome including audiological outcome in children with bacterial meningitis of all causes(11). Previously, a double blind, placebo-controlled trial of dexamethasone in 89 children aged 2 months to 12 years from Pakistan(12) and a North American study(13) had led to conclusions very similar to the Malawi trial(11). The study from Pakistan showed higher mortality in the dexamethasone group with no difference in rates of neurological sequelae and hearing impairment between the dexamethasone group and the placebo group(12). These results could be due to the difference in conditions in developing countries such as late presentations of patients, use of antibiotics prior to hospital presentation and absence of culture/latex positivity for microorganisms. Adverse effects of dexamethasone commonly include GI bleeding and secondary fever. In our study however there was no case of secondary fever documented in the dexamethasone group and the incidence of GI bleeding was similar in the dexamethasone and other groups. Glycerol has been found to be associated with adverse effects like vomiting and nausea but in our study the incidence of vomiting in the glycerol and non-glycerol groups were similar(23). The frequency of hearing sequelae in our study was similar to that (10%) reported from developed countries(1,3), but was significantly lower than that (28%) reported recently from another institution in our region(29). These differences could perhaps be due to better monitoring and treatment facilities available in a tertiary care setting. The strengths of this study were that it was a four-limbed, placebo controlled, double blinded study with 100% follow-up (albeit till 1 month). The study has its own share of limitations also. The sample size was small; hence it was underpowered to detect any small differences in the outcomes measured. In conclusion, use of either glycerol or dexamethasone did not have any significant reduction in the neurological sequelae as well as in the hearing sequelae in children with acute bacterial meningitis. These results may be related to patient characteristics, which may be different in developing countries and need to be studied. Contributors: JS collected the data, did initial analysis and helped in writing the paper; PS planned the study protocol, supervised data collection and analysis and writing of the paper; AB redid the data analysis and wrote the paper; PR did the microbial and other laboratory work; SS conceptualized the study, planned the study protocol, supervised data collection, analysis of data and preparation of final manuscript. Source of funding: Nil. Competing interests: Nil.
|
![]()