S. Noel Narayanan, M. Zulfikar Ahamed and M. Safia
From the Departments of Pediatrics and Cardiology, SAT
Hospital, Medical College,
Thiruvananthapuram 695 011, India.
Correspondence to: Dr. S. Noel Narayanan, T.C. 1/1991,
Kumarapuram, Medical College P. O., Thiruvananthapuram 695 011, Kerala,
India. E-mail:
[email protected]
Manuscript received: September 13, 2004, Initial
review completed: October 19, 2004;
Revision accepted: March 31, 2005.
Abstract:
We report 72 patients with Kawasaki disease seen at this Centre over 7
years. Cardiac involvement in the form of mild pancarditis was seen in
28% patients, but disappeared subsequently. Thirteen (18.5%) children
developed coronary artery disease, out of which 4 resolved by the end
of two months and another 6 after one year; 3 patients continued to
show coronary artery dilatation and aneurysm formation. Children who
received IV gammaglobulin in full dose within 10 days of onset of
illness, showed no evidence of coronary artery disease during follow
up.
Key words: Coronary aneurysm, IV gammaglobulin, Pancarditis.
Kawasaki disease (KD) is considered a rare
disease in the Indian sub-continent(1). During the last decade an
increased incidence is being seen in Kerala(2). Since its original
description by Kawasaki in Japan, KD has been reported from all parts
of the world. The basic pathology is a vasculitis involving all blood
vessels, predominantly the coronary arteries. The diagnosis is based
on easily recognizable clinical features. Five days of fever and at
least 4 of the following 5 principal clinical features should be
present to make a diagnosis of KD(3). These include cervical
lymphadenopathy, a polymorphous rash, ororpharyngeal changes,
bilateral non-purulent conjunctival injection, and limb changes like
erythema and edema of hands and feet followed by periungual
desquamation. The disease generally lasts for 6 to 8 weeks and new
lesions beyond this period are unlikely.
Atypical KD in which patients have fewer than four
of the five clinical features is being increasingly reported(4).
Cardiac complications are the leading cause of morbidity and
mortality. The etiology of KD is unclear although several compelling
hypotheses point to a common infectious agent and genetic
predisposition, resulting in an altered immune response(5). A single
intravenous (IV) infusion of 2 g/kg immunoglobulin is recommended in
addition to high dose aspirin in the first 10 days of the illness, in
patients suspected to have KD(6).
Subjects and Methods
This is a retrospective study of 72 children
admitted and treated with clinical diagnosis of KD at Medical College,
Thiruvananthapuram from 1995 to 2001. The diagnosis of KD was based on
American Heart Association criteria(3). Hemoglobin, blood count, ESR,
CRP, platelet count and routine urine examination were done in all
patients. Paul Bunnel test, Widal, IgM antibodies for dengue, Weil’s
antibodies, rheumatoid factor and other relevant investigations were
done if indicated, to differentiate KD from other illnesses with
similar presentation. Chest X-ray and ECG were done in children
showing positive findings on clinical examination of the
cardiovascular system. A Consultant of Pediatric Cardiology (MZA) did
echo-cardiography at the time of admission during the acute phase and
again at the end of convalescent phase at 8 weeks. Children showing
coronary artery disease were followed up and a third echo-cardiography
was done at the end of one year.
Results
Of 72 patients, 68 met the full diagnostic criteria
for KD. Four had atypical KD with less than four principal clinical
criteria. These atypical cases had strong laboratory evidence to
support a diagnosis of KD and also showed the classical periungual
desquamation. The youngest patient was 5 months old and the oldest 8
years; boys outnumbered girls by ratio of 2.6:1. An adolescent boy in
whom the diagnosis of KD was missed at 7 years of age, later presented
at 15 years with recurrent cardiac syncope, caused by severe coronary
artery disease.
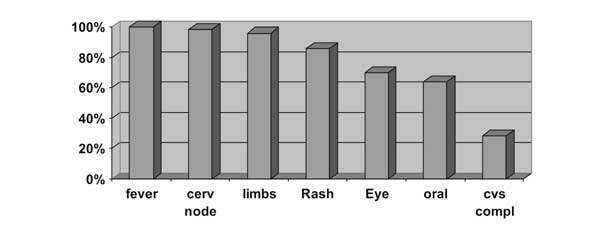
Distribution of clinical features is shown in Fig.
1. Fever of more than 5 days duration was present in 100% children.
Cervical lymph-adenopathy was the commonest finding and oral changes
the least common. Other significant findings were arthritis or
arthralgia, extreme irritability and gastrointestinal symptoms. Two
children developed a second attack of KD. ESR was high in all cases
and 22% had ESR above 100 mm/h. CRP, done in 66 cases, was positive in
80%. Platelet count was significantly raised above 500 × 109/L in 25%
cases. Normal platelet counts were seen in 15% cases and
thrombocytopenia in 2.7%.
 |
|
Fig. 1. Clinical features in patients with
Kawasaki disease. Cerv: cervical lymph; CVS compl:
cardiovascular complications. |
Twenty (28%) children showed abnormal findings in
the heart during the acute stage, in the form of tachycardia, gallop
rhythm, soft apical systolic murmur and muffled first heart sound.
Initial echocardiography showed minimal pericardial effusion in 5
patients, mild valvular leak in 3 and left ventricular dys-function in
one child. All these findings disappeared during convalescence. No
patient had congestive heart failure or arrhythmia. Two of these
patients subsequently developed coronary artery disease which later
resolved by 1 year. Chest X-rays were normal in all cases and ECG
showed minor abnormalities like tachycardia and low amplitude T waves.
On echocardiography, all except one child had
normal left ventricular function. One patient showed decreased
ejection fraction which improved during convalescence. Abnormal
coronary arteries showing either ectasia or aneurysms were found in
thirteen (18.5%) children. Left coronary artery (LCA) was involved in
all cases. Left anterior descending (LAD) was affected in 30% and
right coronary artery (RCA) in 15% cases. There were no circumflex
artery lesions. An adolescent boy, who developed severe coronary
artery disease, was subjected to coronary angiography after an attack
of cardiac syncope. This demonstrated total occlusion of LCA with
calcification, multiple aneurysms and stenosis affecting right
coronary artery (RCA) and presence of prominent collaterals (Fig. 3).
 |
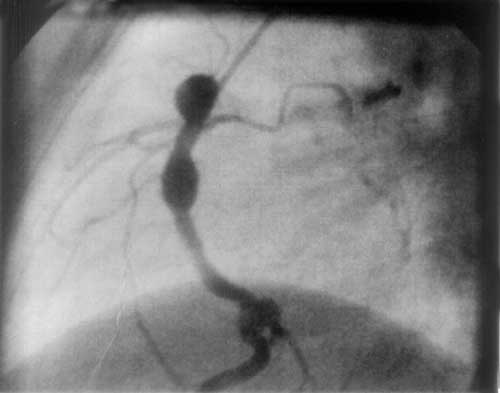 |
Fig. 2. Echocardiography
showing dilated left coronary artery.
|
Fig. 3. Aneurysm and stenosis
affecting right coronary artery and obliterated left anterior
descending. |
IV gammaglobulin was administered in 75% cases
only. Full dose of 2 g/kg/d was given to 55%, and the rest received a
dose of 200 to 400 mg/kg/d for one to two days. Eighteen children
(25%) did not receive IV immunoglobulin due to financial and other
reasons like late presentation or missed diagnosis. Of these 6 showed
coronary artery disease, four of which regressed by one year, while
two are still persisting. Forty children received full dose of IV
immunoglobulin within 10 days of onset of disease. Three of these
children showed mild coronary ectasia during the acute stage. These
resolved on subsequent follow up at 8 weeks. Of 14 patients who
received suboptimal dose of intravenous immunoglobulin, four showed
coronary artery dilatation, three of which resolved at one year and
one persisted. Allergic reaction to IV gammaglobulin in the form of
urticaria and hypotension was observed in four children.
Aspirin was given at a dose of 80-100 mg/kg/d in
four divided doses during the acute phase to all children.
Subsequently a dose of 3-5 mg/kg/d was continued till the end of
convalescent period. In children showing coronary artery disease, low
dose aspirin was continued for more than one year. An
antistaphylococcal antibiotic was given in the acute phase to all
children, in view of the reports of a possible association of toxic
shock syndrome producing staphylococcal infection and KD(7).
Patients with cardiac involvement were followed up
with echocardiography at one year, for vascular and other
abnormalities including valvar leak, pericardial effusion and left
ventricular dysfunction. Thirteen (18.5%) children developed
significant dilatation of coronary arteries. These subsided in 4
children by the end of two months and in another 6 by one year. Three
children, including the adolescent with missed KD, continued to show
coronary aneurysms. There were no deaths. However, the condition of
the adolescent boy with severe coronary artery disease is unstable,
and may require cardiac revascularization in the future.
Discussion
Increased incidence of KD is being seen in Kerala
since 1995. Increased awareness and possibly some unidentified
infectious agent or a genetic susceptibility could explain this
phenomenon. In the present study of 72 children with KD, 28.5% showed
mild pan-carditis during the acute stage. These findings disappeared
by the end of convalescent phase without any sequel. Two of these
children subsequently developed coronary artery lesions, which later
resolved. Coronary artery abnormalities in the form of ectasia or
aneurysm were detected in 18.5% patients on echocardiography. Rowley,
et al. reported coronary artery abnormalities in 20 to 25 % of
children with KD(8). In the present series 40 subjects received IV
gamma-globulin in full dose within 10 days and none of them showed any
coronary artery disease at the end of eight weeks. Coronary artery
dilatation disappeared in four (30%) children by eight weeks and in
another six (46%) by one year. Only 3 (23%) children showed persistent
coronary artery aneurysms beyond one year. Long term follow up of
children with coronary artery aneurysm showed that at least 50%
resolved within 5 to 18 months(9,10). Burns, et al. have reported 74
adult patients with coronary artery disease, which were attributed to
childhood KD(11). As per the guidelines of the American Heart
Association Committee on Rheumatic fever, Endocarditis and Kawasaki
diseases, the adolescent with multiple coronary aneurysms is likely to
require surgery for coronary re-vascularisation(12). At least 13
cardiac trans-plantations have been done so far in patients with KD
and chronic deteriorating left ventricular function(13). A nationwide
survey on KD in Japan showed that the mortality from coronary artery
disease decreased from 1% in 1974 to 0.04% in 1992(14). There were no
deaths in our series.
KD is an emerging disease and increased awareness
among doctors regarding early recognition is important. Clinical
diagnosis is not difficult and timely treatment can prevent
potentially life threatening cardiac complications. A collaborative
study on mortality rate in KD revealed that only boys with cardiac
involvement showed an increase in mortality rate(15). Recent reports
of early and accelerated atherogenesis occurring in arteries affected
by KD as measured by elevated levels of inflammatory markers is of
great concern, since this could accelerate ischemic heart disease in
young adults(16).
Contributors: MS collected and analyzed the data.
MZA did cardiac evaluation and echocardiography and revised the
manuscript critically. SNN supervised the data collection and
analysis, wrote the manuscript and will act as guarantor for the same.
Funding: None.
Competing interests: None stated.
