|
|
Brief Reports Indian Pediatrics 2004; 41:927-937 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Category based Treatment of Tuberculosis in Children |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
S. K. Kabra, Rakesh Lodha and V. Seth From the Department of Pediatrics, All India Institute of Medical Sciences, New Delhi 110029, India. Correspondence to: Dr. S. K. Kabra, Additional
Professor, Department of Pediatrics, All India Institute of Medical
Sciences, New Delhi 110029, India. Manuscript received: July 15, 2003, Initial review
completed: October 8, 2003;
Childhood tuberculosis is treated with multiple regimens for different clinical manifestations. World Health Organization has suggested a category-based treatment of tuberculosis that focuses on adult type of illness. To include children as DOTS beneficiaries, there is a need to assess the feasibility of classification and treatment of various types of childhood tuberculosis in different categories. Methods: The study was conducted in the Pediatric Tuberculosis (TB) Clinic of a tertiary care hospital in North India. All children registered in the TB clinic were classified in four categories, similar to the categorization in World Health Organization’s guidelines for treatment of tuberculosis in adults. All children with freshly diagnosed serious form of tuberculosis were included in category I. Category II included patients who had treatment failure, had interrupted treatment, relapse cases and those who were suspected to have drug resistant tuberculosis. Patients with primary pulmonary complex (PPC), single lymph node tuberculosis, minimal pleural effusion and isolated skin tuberculosis were included in category III. Category IV included patients who did not improve or deteriorated despite administration of 5 drugs (as per Category II) for at least 2 months. Results: A total of 459 patients were started on antituberculosis drugs and were available for analysis. Pulmonary tuberculosis was the commonest followed by lymph node tuberculosis. Identification of AFB was possible only in 52 (11 %) of the patients and was more commonly seen in lymph node tuberculosis. The mean age of the children was 93 months and sex distribution was almost equal. 323 patients were in category I, 12 in category II, 120 in category III and 4 in category IV. 365 (80%) children completed the treatment. Of these, 302 (82.7%) were cured with the primary regimen assigned to them in the beginning, 54 (14.8%) required extension of treatment for 3 months and 9 (2.5%) patients required change in the treatment regimen. Side effect in form of hepatotoxicity was observed in 12 (2.6%) patients and was significantly more in patients who were getting category IV treatment. Conclusion: It is feasible to classify and manage various types of tuberculosis in children in different categories similar to WHO guidelines for adult tuberculosis. Tuberculosis in children is an important cause of morbidity. Diagnosis is often difficult and is based on indirect evidence of infection due to Mycobacterium tuberculosis(1). Clinical symptoms are varied and non-specific due to varied clinical manifestations. For treatment, multiple regimens for different clinical manifestations are in use. Various professional bodies have published standardized treatment of various types of tuberculosis in children according to clinical manifestation(2-5). World health Organization has suggested a category-based treatment of tuberculosis(6). This categorization focuses on adult type of tuberculosis and does not define various types of tuberculosis in children. DOTS strategy aims at treatment of adult patients, particularly, to prevent spread of infection. While tuberculosis in children may not contribute significantly to spread of infection in the community, it remains an important cause of morbidity and mortality. Therefore, it would be desirable to include children as beneficiaries of the DOTS strategy. We conducted a study to evaluate the feasibility of classification and treatment of various types of tuberculosis in children in line with the existing World Health Organization’s proposed DOTS strategy for adults. Subjects and Methods The study was carried out in Pediatric Tuberculosis (TB) Clinic of All India Institute of Medical Sciences, a tertiary care hospital in north India. In our hospital, children with diagnosis of tuberculosis or strongly suspected to be suffering from tuberculosis in Pediatric general out patient services (OPD) are referred to Pediatric Tuberculosis Clinic for opinion and further treatment. All the children registered in the clinic are subjected to detailed history, physical examination and investigations (if not done before referral). The diagnosis is made on the basis of protocol being followed in the clinic. Those who attend the clinic for second opinion are referred back to their primary care facilities. Those judged not to have tuberculosis are sent back to Pediatric OPD for further management. Children with definite tuberculosis attend the clinic every 4 weeks. All children registered in the TB clinic from January 2000 to June 2002 were classified into four categories as per Table I. The categorization was based on World Health Organization’s guidelines for the treatment of tuberculosis in adults(6). All freshly diagnosed serious cases of tuberculosis were included in category I. In addition, patients with joint tuberculosis were also included in category I, because it may have long-term sequlae, if treated inadequately producing handicaps later in life. Children who received full antituberculosis treatment in past and were declared cured and presented again with tuberculosis disease (relapse cases) were included in category II. Patients who were diagnosed to have tuberculosis in the past and received irregular treatment for the same without improvement or deteriorated (suspected resistance) were also placed in category II. A child who failed to respond or deteriorated (clinical/ radiographic evidence+ bacteriology) after 12 weeks of intensive phase with good compliance was defined as treatment failure and placed in category II. Patients who interrupted treatment for two months or more, and returned with active TB as judged on clinical and radiological assessment (treatment after interruption) were also classified in category II. Patients with primary pulmonary complex (PPC), single lymph node tuberculosis, minimal pleural effusion and isolated skin tuberculosis were included in category III. Category IV included patients who did not improve or deteriorated despite administration of 5 drugs (as per category II) for at least 2 months. Table I Clinical Categories and Clinical Conditions in Children.
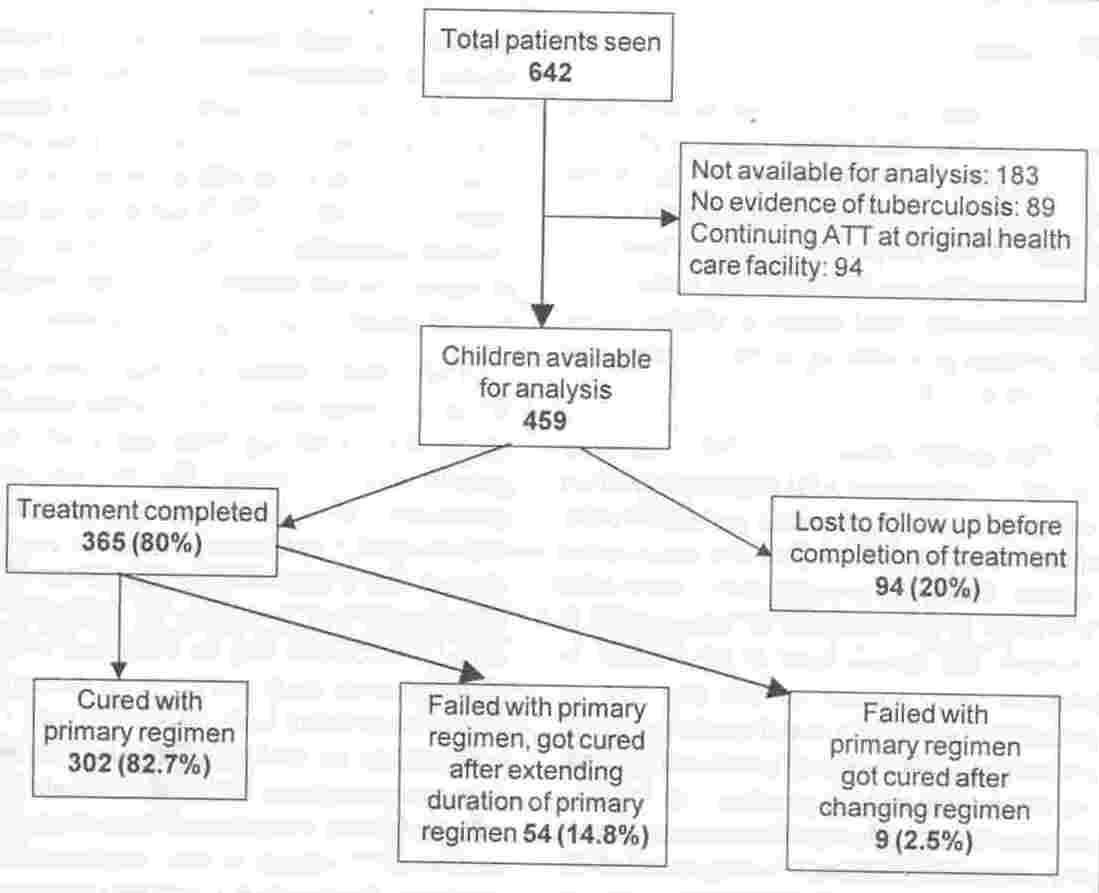
PPC- Pulmonary Primary Complex, PPD- Progressive Primary Disease, TBL- Tubercular Lymphadenitis, CNS TB- Central Nervous System Tuberculosis, 2HRZE 4HR- 2 months of isoniazid, rifampicin, pyrazinamide and ethambutol, followed by 4 months of isoniazid and rifampicin, 2SHRZE 1 HRZE 5HRE- first two months daily isoniazid, rifampicin, pyrazinamide, ethambutol and streptomycin followed by one month of isoniazid, rifampicin, pyrazinamide and ethambutol, followed by 5 months of isoniazid, rifampicin and ethambutol, 2HRZ 4HR - 2 months of isoniazid, rifampicin and pyrazinamide, followed by 4 months of isoniazid and rifampicin. * 10 HR in cases of Osteoarticular and CNS tuberculosis. ** Treatment with at least 3 new drugs that patient has not received in the past and to continue the drugs for 24 months. Diagnosis of pulmonary tuberculosis was based on clinical presentation (including family history), abnormal chest X-ray (CXR) film with positive Mantoux test (using 5 TU PPD-S) or non-clearance of CXR after a course of antibiotics. Depending on the CXR picture, a diagnosis of primary pulmonary complex (PPC), progressive primary disease (PPD), cavitatory tuberculosis or pleural effusion was made. The diagnosis of lymph node tuberculosis (TBL) was based on findings of fine needle aspiration cytology (FNAC)(7). Abdominal tuberculosis was diagnosed with abnormal ultrasonography/ barium studies and positive Mantoux test or abdominal lymph node biopsy (done in patients who under- went laparotomy for intestinal obstruction) suggestive of TB. Osteoarticular TB was diagnosed when imaging studies were suggestive of tuberculosis, with evidence of TB infection in form of positive Mantoux test and/or histologic/cytologic findings on synovial biopsy or joint fluid suggestive of tuberculosis. CNS TB was diagnosed in children with neurological manifestations and suggestive findings on cerebrospinal fluid examination, neuroimaging and evidence of TB infection (positive Mantoux test). A diagnosis of disseminated tuberculosis was made when there was evidence of tuberculosis from at least two anatomically different sites. A diagnosis of tubercular pericarditis was made in the presence of positive Mantoux test with pericardial effusion and absence of other possible causes of pericardial effusion. Diagnosis of genitourinary tuberculosis was based on demonstration of Mycobacterium tuberculosis in urine on culture. Patients in category I were treated with 2 months of isoniazid, rifampicin, pyrazinamide and ethambutol, followed by 4 months of isoniazid and rifampicin (2HRZE 4HR). Patients with CNS TB and osteoarticular TB were treated with 2HRZE 10HR. For category II patients in the first two months isoniazid, rifampicin, pyrazinamide, ethambutol and streptomycin were given daily followed by one month of isoniazid, rifampicin, pyrazinamide and ethambutol, followed by 5 months of isoniazid, rifampicin and ethambutol (2SHRZE/1HRZE/5HR). Patients in category III were treated with 2 months of isoniazid, rifampicin and pyrazinamide, followed by 4 months of isoniazid and rifampicin (2HRZ/ 4HR). Patients in category IV were treated with at least 3 new drugs that they had not received in past, and the drugs were continued for 24 months. We followed daily regimen in place of intermittent regimen, as the treatment was not directly observed. Doses of isoniazid were 5-7 mg/kg/day, rifampicin 10-12 mg/kg/day, pyrazin-amide 25-30 mg/kg, ethambutol 15-20 mg/kg/day and streptomycin 20 mg/kg/day. All enrolled children were followed up every four weeks. On each visit the child was examined for clinical improvement, weight gain, and side effects of medications. Parents or caretakers were asked about the compliance of the treatment. If a child developed some adverse drug reaction, they were treated according to standard treatment protocol(8). Outcome of patients was assessed as cured, extension of treatment or change in regimen or lost to follow-up. Cure was defined as absence of clinical symptoms with regression of X-ray finding of > 2/3 of the original lesion after the assigned treatment, wherever there were radiologic abnormalities at the time of diagnosis. Extension of treatment was considered when a patient was continued on maintenance treatment for more than assigned duration in the beginning. The duration was extended by 3 months in children suffering from pulmonary tuberculosis and their CXR did not show resolution of lesion by >2/3 of the initial lesion In children with TB lymphadenitis (TBL) treatment was extended by 3 months in patients who developed fresh lymph nodes or size of lymph node increased during treatment. Change in antituberculosis treatment regimen was considered when whole regimen was changed from the one assigned in the beginning. This was done if there was worsening or no improvement in the clinical and/or radiologic features even after 2 months of intensive phase. Those who did not complete assigned treatment were considered as lost to follow-up. Results During the study period 642 patients were referred to the Tuberculosis clinic. After assessment 89 children were found not to have tuberculosis. Ninety-four patients came only for second opinion and were sent back to their primary health care facility for completion of treatment. A total of 459 patients were started on antituberculosis drugs and were available for analysis. 365 patients completed the treatment and 94 did not complete the treatment (Fig. 1). The mean follow up for 365 patients who completed the treatment was 9.1 + 3.45 months (median 8 months 95% CI; 8-9 months). The mean follow up of patients who did not complete the treatment was 2.7 + 1.9 months (median 2 months; 95% CI 2-3 months).
The mean age of children referred to TB clinic was 93 months and sex distribution was almost equal (Table II). Table II Age and Sex Distribution of Children with Tuberculosis.
CI: confidence interval. Of the 459 patients, 323 patients were in category I, 12 were in category II, 120 in category III and 4 in category IV. Pulmonary tuberculosis was the commonest followed by lymph node tuberculosis. The type of tuberculosis and treatment category along with their outcome is shown in Table III. Table III Outcome of Patients in Different forms of Tuberculosis
PPC - Pulmonary Primary Complex, PPD - Progressive Primary Disease. TBL- Tubercular Lymphadenitis, CNS TB- Central Nervous System Tuberculosis. *Outcome- I: cure with primary regimen, II: Failed with primary regimen achieved cure after extension of treatment, III: Failed with primary regimen achieved cure after change in regimen, IV: lost to follow up.
Of the total 459 patients available for follow up, 365 (80%) completed the treatment. Of the 365 patients who completed treatment, 302 (82.7%) were cured with the primary regimen assigned to them in the beginning. Sixty-three (17%) patients failed to get cured with the primary regimen. Of them 54 (14.8%) got cured with extension of treatment for 3 months and 9 (2.5%) patients required change in the treatment regimen. Isolation of AFB was possible only in 52 (11 %) of the patients and was more commonly seen in lymph node tuberculosis (Table IV). Table IV AFB Positivity and Type of Tuberculosis
PPC - Pulmonary Primary Complex, PPD - Progressive Primary Disease, TBL - Tubercular Lymphadenitis. Side effect in form of hepatotoxicity was observed in 12 (2.6%) patients and were significantly more in patients who were getting category IV treatment (Table V). Table V Drug Induced Hepatitis in Different Category of Patients.
Discussion An attempt has been made to develop a model of treatment for tuberculosis in children in lines with that suggested by World Health Organization for treatment of tuberculosis in adults. While preparing treatment protocol, recommendations of professional bodies(2-5) and various reports of treatment of tuberculosis in children available in literature were also consulted(9-19). The modifications in WHO guidelines included: inclusion of AFB negative patients in category 1. WHO guideline includes freshly diagnosed AFB positive and AFB negative but serious illness in category I(6). Since AFB positivity is less common in tuberculosis in children, the serious form of tuberculosis in children was defined as one that can be identified objectively based on X-ray film of chest in pulmonary tuberculosis and by other objective criteria depending on organs involved and subsequent outcome. Other important difference was treatment with daily regimens rather than intermittent regimen because the treatment in this study was not directly observed. Success of intermittent regimen has been demonstrated in various studies in children(9-13). With our observa-tions of feasibility of categorization of tuber-culosis in children into existing framework available for adults and efficacy of intermittent regimens, it should be feasible to include children as beneficiaries of the DOTS strategy. However, this will require appropriate formula-tions of antituberculosis drugs for children. The other difference was prolonged duration of treatment up to 12 months when the illness was involving bone and joints and central nervous system. The recommended guidelines of professional bodies were followed(3-5). However, recent studies suggest that 6 months of treatment for CNS tuberculosis and 9 months of treatment in spinal tuberculosis may be sufficient(14-17). Aim of present study was to see the feasibility of categorization of various types of tuberculosis in children and not to study appropriate regimen for treatment and that’s why we followed current recommendations of various professional bodies on duration of treatment. Further studies with shorter duration of treatment may give more confidence and duration of treatment may be reduced in future. Ethambutol was used for all age groups in categories I and II. It was based on the reports and recommendations that it can be used in doses of 15-20 mg/kg in young children without significant increase in the ocular toxicity(18-19). In the present study, the diagnosis was often based on indirect evidence of infection due to Mycobacterium tuberculosis as AFB could be demonstrated only in 11% of the patients. Poor yield of AFB in tuberculosis in children may be due to paucibacillary nature of illness and inability of young children to give appropriate sputum samples. Children in our study were investigated and treated on ambulatory basis and no extra effort was made for isolation of AFB. The yield of AFB in children with pulmonary tuberculosis can be improved by induction and collection of sputum(20). In this study, 80% of the patients completed the treatment without active follow up. We could not find similar study on children in literature for comparison. A reasonably good case holding in our study was because of the following factors: (i) patients were regularly followed up on a specified day in a specialty clinic; (ii) some of the drugs (isoniazid, rifampicin and pyrazinamide) were provided to patients (given by non-governmental organization) free by regular staff of our hospital and (iii) the medicines were available without break. Case holding in our patients could have been better if all medications were provided and a regular contact was made for those who did not come for follow up. The overall cure rate with primary treatment regimen was 98%. Cure rate of chemotherapy for different types of tuber-culosis in various reports vary from 80-100%(9-17, 21-24). The duration of treatment was extended in 54 (15%) patients. Decision to extend the treatment in pulmonary tuberculosis was based on non-resolution of clinical and CXR finding. However, non-resolution of CXR finding may not always suggest active disease(25,26). Extension of treatment in children with TBL was based on appearance of fresh lymph nodes or increase in size of lymph node during treatment. Enlargement of lymph node or appearance of new lymph node during treatment may be because of delayed type of hypersensitivity (DTH) reaction or a resistance type of tuberculosis(27). In the absence of definitive test for identification of either possibility the maintenance treatment was extended. It is felt that there is a need for guidelines about extension of treatment in various types of tuberculosis. Side effect in the form of hepatitis was observed in 2.6% of patient. Hepatitis has been reported in 2-10% of the children on antituberculosis drugs(28-29). There are a few limitations of the present study. It is a hospital-based study carried out in a tertiary care referral center and may not represent proportion of different type of tuberculosis in a community or a general hospital. However, it gives an idea about feasibility of categorization and success rate of treatment for any set up. Almost 15% of children referred with a diagnosis of tuberculosis, actually did not appear to have the disease; this emphasizes the need for caution in diagnosis of tuberculosis in children. To reduce the chances of under- and over-diagnoses, it is important to have personnel trained in this field. As the mean follow up was just above 9 months, relapse rates cannot be commented upon. Prior to year 2000 we were treating children with tuberculosis as per guideline of Indian Academy of Pediatrics(2). In this guideline patients were classified into 5 groups. This was a comprehensive protocol as it included guideline for treatment of various types of tuberculosis as well as preventive therapy but the number of groups was 5. The WHO guideline does not include preventive therapy but has only 3 categories therefore easy to remember. WHO guideline is being implemented for adults as part of DOTS strategy. Formulation of similar classification for children may make inclusion of children in DOTS more feasible and all patients with tuberculosis in community can then be managed under the same program. From this study, it is inferred that it is feasible to classify and treat different type of tuberculosis in children in different categories based on WHO guidelines for adult tuber-culosis. Despite limitations, our data will help in planning similar studies and arriving at a consensus for category based treatment of tuberculosis in children and inclusion of children as beneficiaries of DOTS. Acknowledgement We are thankful to IC Trust, New Delhi for providing antituberculosis drugs for distribution to patients attending the Tuberculosis Clinic. Contributors: SKK and RL involved in design, data collection and manuscript writing; SKK will act as guarantor for the paper. VS was involved in design of study and manuscript writing. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()