|
|
|
Indian Pediatr 2019;56: 799 |
 |
Teenager
with Cystic Swelling in the Floor of the Mouth
|
|
Indar Kumar Sharawat 1,
Arun Kumar2 and
Lesa Dawman3
From Departments of 1Pediatrics and 2Oral
health, PGIMER Satellite Centre, Una, Himachal Pradesh; and 3Department
of Pediatrics, PGIMER, Chandigarh; India.
Email: 3
[email protected]
|
|
A 15-year-old girl presented with complaint of progressively increasing
swelling in the right side of the floor of mouth for the past one and
half month. It was not associated with pain, but patient had difficulty
in swallowing and mastication. On examination, there was a dome shaped,
painless, bluish, well-circumscribed, fluctuating, non-compressible
cystic swelling measuring 3.5 × 3.0 cm on the right side of the floor of
mouth, pushing the lingual frenulum to left side and causing elevation
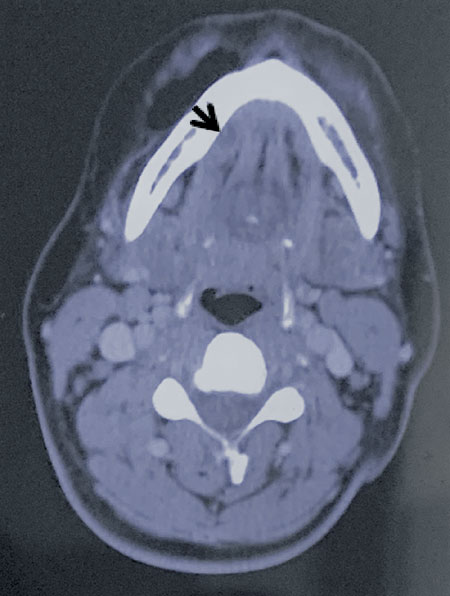
of tongue (Fig. 1). Contrast-enhanced computed tomography
showed a thin-walled cystic lesion at the floor of the mouth (Fig.
2) without any obstruction or cervical extension, suggesting a
diagnosis of ranula.
 |
|
Fig.1 Dome-shaped bluish, well
circumscribed, semi-transparent, cystic swelling measuring 3.5 ×
3 cm on the right side of floor of the mouth, pushing the
lingual frenum to left side.
|
 |
|
Fig. 2 Contrast enhanced CT of floor
of the mouth (axial section) shows an enhancing cystic
lesion measuring, involving right floor of the mouth, abutting
medially the right geniohyoid, genioglossus and the mylohyoid
muscles (arrow).
|
Other differential diagnoses of cystic lesions at the
floor of the mouth are ranula, dermoid and epidermoid cysts (soft
nodular lesions with sessile base), lipoma (asymptomatic yellowish mass
with doughy feel), vascular/lymphatic malformations (usually in infants,
soft and compressible mass), Wharton duct blockage (pain and swelling of
the affected salivary gland which get worse with chewing and smell of
food), infections (painful, fever, adenopathy and associated dysphagia),
and neoplasms of the salivary glands (rare in children, painful). This
cystic lesion was consistent with typical appearance of an oral ranula
(dome shaped, unilateral, painless, bluish, well-circumscribed,
semi-transparent, fluctuating, and non-compressible cystic swelling).
Based on their location, ranulae are divided into three groups:
sublingual, sublingual-submandibular and submandibular. Sublingual
ranula is a pseudocyst formed by extravasation and subsequent collection
of the mucoid saliva from the submandibular gland. Females are more
commonly affected, and usually present between first and second decade
of the life. Formation of the ranula is attributed to the traumatic
rupture of the salivary duct. Ranula may be asymptomatic, may have
intermittent shrinkage, or can progress to a large lesion interfering
with swallowing and articulation. Associated secondary bacterial
infection may cause pain and tenderness. Treatment is required in large
and symptomatic ranula. Marsupialization was previously used technique,
but with high (60-90%) recurrence rate. Removal of the cyst along with
sublingual gland is the preferred surgical method.
|
|
|
 |
|
