|
|
|
Indian Pediatr 2016;53: 793-795 |
 |
Ultrasonographic Confirmation of Endotracheal Tube Position in
Neonates
|
|
Khadijehsadat Najib, Narjes Pishva, Hamid Amoozegar,
#Parisa Pishdad
and $Ebrahim
Fallahzadeh
From Neonatal Research Center, *Pediatric Cardiology
Services, #Department of Radiology, and $Gastroenterohepathology
Research Center; Shiraz University Of Medical Sciences, Shiraz, Iran.
Correspondence to: Dr Parisa Pishdad, Medical Imaging
Research Center, Shiraz University Medical Center, Shiraz, Iran 71365.
Email: [email protected]
Received: July 09, 2015;
Initial review: October 09, 2015;
Accepted: August 01, 2016.
|
Objective: To compare endotracheal tube tip-to-carina distance
obtained by ultrasonography vs. that obtained by chest X-ray
in neonates.
Methods: After endotracheal intubation of 40
neonates, chest X-ray and, within one hour, ultrasonography was
obtained for each patient for measurement of endotracheal tube
tip-to-carina distance.
Results: Means of endotracheal tube tip-to-carina
distances were not significantly different by both modalities (mean
difference 0.157 cm, P= 0.06). In addition, an intraclass
correlation was observed between them (r2= 0.61, 95% CI= 0.26, 0.79).
Conclusion: Ultrasonography and chest X-ray
are equally accurate for determination of endotracheal tube
tip-to-carina in infants. As ultrasonography is more easily available
and is safer than X-ray, it may be a better modality for
confirming proper placement of endotracheal tube in neonates.
Keywords: Endotratracheal intubation, Radiography,
Ultrasonography.
|
|
Clinical evaluation, radiography, ultrasonography
(US), exhaled carbon dioxide detection and bronchoscopy are some
methods to diagnose misplaced intubation [1-3]. Schmolzer, et al.
[4] reported that chest radiography is the gold standard method for
endotracheal tube (ET) positioning. However, the toil, the time needed,
and X-ray exposure required for radiographic assessment of ETT
position have caused investigators to consider whether US could be
equally useful in this regard [5-11].
Currently, in our center, chest X-ray is the
standard method for the evaluation of the endotracheal tube position.
This is obtained following each neonatal intubation (primary or after
re-intubation). Considering the potential disadvantages of radiography,
we decided to evaluate US as an alternative method for tube
localization.
Methods
This cross-sectional study was carried out in infants
admitted to neonatal intensive care unit (NICU) of Namazee, Hafez and
Zeinabiyeh hospitals affiliated to Shiraz University of Medical
Sciences, Iran, from May to October 2014. We included all admitted
infants who required intubation. Infants whose ETT tip was not clearly
visible by any modality were not included in the study.
CXR was obtained for each neonate after primary
intubation or re-intubation. Proper site of the ET tip on CXR was
defined as below the thoracic inlet and above the carina. All infants
underwent portable US (by Teknova TH-5100) within 1h of chest X-ray.
Midsagittal views were obtained by a high-frequency linear probe (10
MHZ) for evaluation of ET-tip distance from superior portion of the
right pulmonary artery, the anatomic equivalent of the carina. US was
performed under the supervision of a radiologist or a pediatric
cardiologist, by a neonatologist who had been trained for chest
sonography for at least 6 months prior to the time of the study. All
operators were unaware of the result of radiographic assessment of ET
position. The ET could be moved in and out about 2 mm for better
visualization of the tip position. The distance of ET-tip to carina on
chest X-ray was measured by a radiologist who was blinded to
sonographic findings. The time required to obtain both the
investigations was recorded for each patient.
This study was approved by Institutional ethical
committee of Shiraz University of Medical Sciences. SPSS
(V.16) was used for statistical analysis.
Results
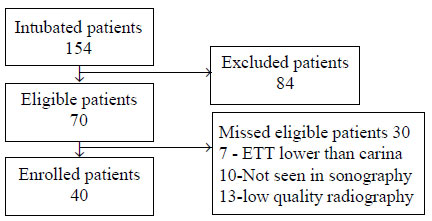
A total of 154 infants were admitted and intubated in
the NICU during the 6 month study period. Of the 70 eligible patients,
thirty were excluded from the study due to ET tip lower than the carina
(7 patients) or ET tip higher than the thoracic inlet (10 patients), and
improper radiography technique (13 patients) (Fig. 1).
Forty infants (24 males) were finally enrolled. Mean (SD) age of
included infants was 16 (17) days (median: 8 d, range: 1 to 64 d). Seven
patients who had chronic lung disease (17.5%) were beyond neonatal age.
Mean (SD) weight and length were 2037 (924) grams and 42.5 (6.6) cm,
respectively.
 |
|
Fig. 1 Flow of patients in study.
|
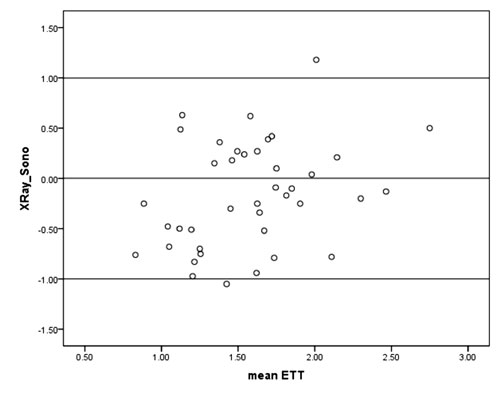
Mean (SD) distance of ET tip-to-carina (or RPA) was
1.49 (0.5) and 1.65 (0.4) centimeters on CXR and US, respectively.
Differences between ET tip-to-carina values measured by radiography
versus those obtained by US were not significant (mean difference 0.157
cm, P= 0.067). An intraclass correlation (ICC) was observed
between ETT tip-to-carina distance on US and CXR (r 2=
0.61, 95% CI= 0.26, 0.79) displays the Bland-Attman plot of ET-to-Carina
distance as measured by two methods (r2=0.314).
 |
|
Fig. 2 Bland-Altman plot of distance
measured by sonography versus radiography between endotracheal
tube and carina.
|
Mean (SD) time interval between intubation and
radiographic evaluation was 2 (1) hours while the required time for US
assessment was less than 5 minutes.
Discussion
Identification of an appropriate method for
evaluation of ET position is very important; finding a fast and simple
method should be considered necessary. Results from this study showed
that both US and chest X-ray have similar accuracy in evaluation
of ET tip-to-carina distance.
Although some previous studies imply that chest X-ray
is a good method for evaluation of ET positioning [7,12] others have
proposed that US is even better for this purpose [8-11,13]. Dennington,
et al.[7] showed that bedside US has a relatively good
correlation with radiography (r2=
0.68) which is comparable with our study. We observed an accuracy of
100% in detection of ET tip by sonography. This study also provided
evidence of considerable time advantage of US over chest X-ray.
Data from a majority of studies in this field is in agreement with our
study [4,8,13-15].
Our study has limitation of a small sample size. Time
interval between radiography and sonography was up to 1 h; a shorter
interval would have produced more valid results.
In conclusion, US and chest X-ray are equally
accurate for determination of ET tip-to-carina in neonates requiring
endotracheal intubation. As US is more easily available and is faster
and safer than X-ray, may be considered a better modality for
this purpose.
Contributors: All authors contributed to
contributions to the conception and design of the work; the acquisition,
analysis, and interpretation of data; drafting the work; and final
approval of the version to be published. Funding: None;
Competing interest: None stated.
|
What This Study Adds?
•
Ultrasonography is a valid
method for the assessment of endotracheal tube tip position in
neonates.
|
References
1. Timmermann A, Russo SG, Eich C, Roessler M, Braun
U, Rosenblatt WH, et al. The out-of-hospital esophageal and
endobronchial intubations performed by emergency physicians. Anesth
Analg. 2007;104:619.
2. Hosono S, Inami I, Fujita H, Minato M, Takahashi
S, Mugishima H. A role of end-tidal CO2 monitoring for assessment of
tracheal intubations in very low birth weight infants during neonatal
resuscitation at birth. J Perinat Med. 2009;37:79.
3. Rudrarajun P, Eisen LA. Confirmation of
endotracheal tube position: A narrative review. J Intensive Care Med.
2009; 24:283-92.
4. Schmölzer GM, O’Reilly M, Davis PG, Cheung PY,
Roehr CC. Confirmation of correct tracheal tube placement in newborn
infants. Resuscitation. 2013;84:731-7.
5. Schmölzer GM, Roehr CC. Techniques to ascertain
correct endotracheal tube placement in neonates. Cochrane Database Syst
Rev. 2014;9:CD010221.
6. Mora-Matilla M, Alonso-Quintela P, Oulego-Erroz I,
Rodríguez-Blanco S, Gautreaux-Minaya S, Mata-Zubillaga D. Is ultrasound
a feasible tool to verify endotracheal tube position in neonates?
Resuscitation. 2013;84:e19-20.
7. Dennington D, Vali P, Finer NN, Kim JH. Ultrasound
confirmation of endotracheal tube position in neonates. Neonatology.
2012;102:185-9.
8. Sethi A, Nimbalkar A, Patel D, Kungwani
A, Nimbalkar S. Point of care ultrasonography for position of tip of
endotracheal tube in neonates. Indian Pediatr. 2014;5: 119-21.
9. Tessaro MO, Salant EP, Arroyo AC, Haines LE, Dickman
E. Tracheal rapid ultrasound saline test (T.R.U.S.T.) for confirming
correct endotracheal tube depth in children.
Resuscitation. 2014;89C:8-12.
10. Weaver B, Lyon M, Blaivas M. Confirmation of
endotracheal tube placement after intubation using the ultrasound
sliding lung sign. Acad Emerg Med. 2006; 13:239-44.
11. Chou HC, Tseng WP, Wang CH, Ma MH, Wang HP, Huang
PC, et al. Tracheal rapid ultrasound exam (T.R.U.E.) for
confirming endotracheal tube placement during emergency intubation.
Resuscitation. 2011;82: 1279-84.
12. Levy FH, Bratton SL, Jardine DS. Routine chest
radiographs following repositioning of endotracheal tubes are necessary
to assess correct position in pediatric patients. Chest.
1994;106:1508-10.
13. Saboo AR, Dutta S, Sodhi KS. Digital palpation of
endotracheal tube tip as a method of confirming endotracheal tube
position in neonates: An open-label, three-armed randomized controlled
trial. Paediatr Anaesth. 2013; 23:934-9.
14. Harris EA, Arheart KL, Penning DH. Endotracheal tube
malposition within the pediatric population: a common event despite
clinical evidence of correct placement. Can J Anaesth. 2008;55:685-90.
15. Bruno M, Pierre F, Anne H, Renée KH, Thomas E,
Bruno B, et al. Airway Management in Children: Ultrasonography
assessment of tracheal intubation in real time? Anesth Analg.
2009;108:461-5.
|
|
|
 |
|
