|
|
Correspondence Indian Pediatrics 2008; 45:864 |
|||
|
Impending Rupture of Splenic Abscess in Enteric Fever |
|||
|
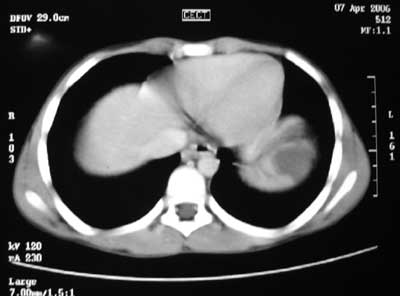
An 11 year-old male child presented with fever and pain in the left upper abdomen for 2 weeks. Patient was febrile and there was tenderness in the left hypochondrium; there was no organomegaly. Leucocyte count was 17,500/mm3. Widal test was positive. Ultrasonography of abdomen showed two well-defined hypoechoic lesions in spleen. CT scan revealed three abscesses in spleen - upper pole (50 mL), middle (20 mL) and lower pole (30 mL). Abscess in the upper pole was abutting the diaphragm and was in danger of rupture (Fig. 1). Splenectomy was planned in view of impending rupture. Postoperative period was uneventful. Pus culture was sterile, AFB and gram stain did not reveal any organism. Histopathology showed necrotic material with infiltrative exudates.
The usual cause of splenic abscess is hematogenous seeding of the spleen from an infective focus elsewhere. A few cases with multiple splenic abscesses caused by S. typhi are described. Allal, et al.(3) reported 400 patients with S. typhi and found splenic abscess in 8 (2%) cases; of these only one had multiple splenic abscess. Percutaneous drainage is indicated for uniloculate solitary abscess without internal debris, septations and in high-risk surgical patients. Splenectomy is required in other situations. If untreated, splenic abscess may rupture and the prognosis in these patients is bleak. Vikas Jindal and V P Singh,
|
![]()