|
|
Case Reports Indian Pediatrics 2008; 45:859-861 |
|||||
|
Sly Disease: Mucopolysaccharidosis Type VII |
|||||
|
Sheela Nampoothiri Kappanayil Mahesh* K R Hiran† V Sunitha From the Department of Pediatric Genetics,*Pediatric Cardiology, and †Pathology, Amrita Institute of Medical Sciences and Research Center, Elamakkara PO, Cochin 682 026, Kerala, India. Correspondence to: Sheela Nampoothiri, Consultant,
Department of Pediatric Genetics, Amrita Institute of Medical Sciences
and Research Center, Elamakkara PO, Cochin 682 026, Kerala, India. Abstract
Mucopolysaccharidosis (MPS VII) (Sly Disease) is a rare lysosomal storage disorder described by Sly, et al. in 1973(1). It is an autosomal recessive disorder caused by the deficiency of b-glucuronidase enzyme, leading to lysosomal storage of heparan, dermatan and chondroitin sulphate. The gene for b-glucuronidase is mapped to 7q 21.2–22. The disease has a variable phenotype from hydrops fetalis to mildly affected adults including the severely affected infants. To the best of our knowledge this is the first case of proven Sly Disease from India. Case Report A 6 month-old female infant presented in the Pediatric Cardiology department with a history of poor weight gain, rapid respiration and interrupted feeding of about one month duration. Her cardiovascular examination revealed severe mitral regurgitation and congestive cardiac failure. Chest X-ray showed cardiomegaly with a cardiothoracic ratio of 70% with normal lung vascularity. ECG indicated left atrial and left ventricular volume overload. Echocardiogram demonstrated thickened mitral valve leaflets with prolapse of the posterior mitral leaflet resulting in severe mitral regurgitation. She was referred to the Genetics department for evaluation of dysmorphic features. She was born to second-degree consanguineous parents. This couple had four pregnancies of which two had ended as first trimester miscarriages. One pregnancy was termi-nated at 7 months as the baby had severe hydrops fetalis. The parents did not entertain postmortem studies. The proband had a birthweight of 2750 g. At 6 months, she had central hypotonia and had not attained head steadiness, but had good cognitive development and could recognize her parents. Her weight was 5.5 kg (<5th centile), length 66 cm (5th centile) and head circumference 40 cm (<5th centile). She had hypertelorism, depressed nasal bridge, epicanthic folds, a long philtrum and thin upper lip, low-set ears with a normally shaped pinna, a small anterior fontanel, and prominent hypertrichosis (Fig. 1). She had a firm hepatomegaly of 6 cm and splenomegaly of 4 cm. She had corneal clouding, confirmed by slit lamp study.
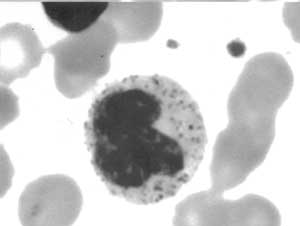
X-ray evaluation revealed broad ribs and ovoid vertebrae, and mild beaking of the second lumbar vertebra. Wrist X-ray showed normal metacarpals with two carpal bones. Pelvis X-ray showed marked hypoplasia of the inferior portions of the ilia, with slanted acetabulae. Peripheral smear examination revealed characteristic Alder-Reilly granules, which are large, purplish-black, coarse azurophilic granules (Fig. 2). 2D electrophoresis of the urine showed a band of dermatan sulphate. Oligosaccharide screening of urine was negative. b-glucuronidase level was 6.4 nmol/hr/mg (normal, 350-500 nmol/hr/mg), which was only 1.8 % of the expected level, confirming the diagnosis of Sly Disease.
Surgical repair of the mitral valve was contemplated, but her parents opted for conservative management. The cardiac status of the child is being periodically monitored. Parents were counseled regarding the feasibility of prenatal diagnosis in future pregnancy following the confirmation of diagnosis of Sly disease in the proband. Discussion Sly Disease is an extremely rare autosomal recessive disorder due to deficiency of b-glucuronidase, and is the least common type of MPS.The major clinical features are postnatal growth retardation, mode-rately severe mental retardation, coarse face, hepatosplenomegaly, corneal clouding, involvement of heart valves, macrocephaly, hydrocephalus, inguinal hernia and joint contractures. Corneal clouding is a feature of the severe form. Dysostosis multiplex is less pronounced than in other mucopolysaccharidoses. Skeletal survey shows flaring of lower ribs, thoracolumbar gibbus, odontoid hypoplasia, and antero-inferior beaking of the lower thoracic and lumbar vertebrae. Peripheral smear evaluation is an extremely useful modality for clinching the diagnosis. Alder Reilly granules are differentiated from toxic granules by their abundance, obscuring of the nuclear morphology in neutrophils, presence in lymphocytes and monocytes, and by lack of clinical evidence of sepsis. These granules are also seen in Maroteaux-Lamy syndrome (MPS VI) and in multiple sulphatase deficiency(2). One peculiar feature of Sly Disease is that unlike other mucopolysaccharidoses, the disease can be recognized in the neonatal period if it is associated with hydrops fetalis. This severe manifestation leads to death within months, whereas in the milder form the patients present with developmental delay and survive into adolescence. Since Sly disease can cause recurrent fetal hydrops and can be confirmed by in utero evaluation of b-glucuronidase levels, it should be included in the panel of investigations for a case of non-immune hydrops fetalis(3). MPS type VII is the most common cause for hydrops fetalis among the mucopolysaccharidoses, though type IV and VI can rarely present with hydrops(4). Two uncommon features in affected fetuses with Sly disease are increased nuchal translucency at first trimester screening and intrauterine growth acceleration leading to advancement of bone age(5,6). Confirmation of prenatal diagnosis is by demonstration of deficiency of b-glucuronidase from the analysis of cultured amniocytes or chorionic villus specimens. Evaluation of amniotic fluid for the 2-D electrophoresis pattern of glycosaminoglycans aids in confirmation of the diagnosis(7). Detection of the mutation by PCR based restriction fragment length polymorphism would allow detection of this mutation for prenatal screening, provided the mutation has already been confirmed in the proband(8). The most common mode of cardiac involvement in MPS is thickening of the mitral valve with regurgitation or stenosis. The mitral valve is more commonly involved than the aortic valve. In majority of patients with MPS in whom dermatan sulphate has accumulated, cardiac involvement was most frequent and severe(9). Mitral valvuloplasty has been successfully done in a child with MPS type III for alleviation of severe mitral regurgitation. Allogenic bone marrow transplantation has significantly improved the motor function, has reduced the frequency of recurrent respiratory infections and also has shown substantial improvement of vertigo, dyspnea and snoring(10). Corneal transplantation is a valuable adjunctive treatment option in patients with severe corneal clouding as bone marrow transplantation does not alleviate or reverse the corneal clouding. Acknowledgment We would like to acknowledge Dr Radha Rama Devi, Consultant, Diagnostic Division, CDFD, Hyderabad for the estimation of b-glucuronidase. Contributors: SN diagnosed the condition in the index case and drafted the article. She will act as the guarantor of the manuscript. MK did the cardiological evaluation of the patient. HKR has evaluated the peripheral smear for confirmation of diagnosis. SV did the literature search and helped in the drafting of the article. Funding: None. Competing interests: None stated. .
|
![]()