|
|
Short Communications Indian Pediatrics 2008; 45: 852-854 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Concerns on the Dosing of Antitubercular Drugs for Children in RNTCP |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
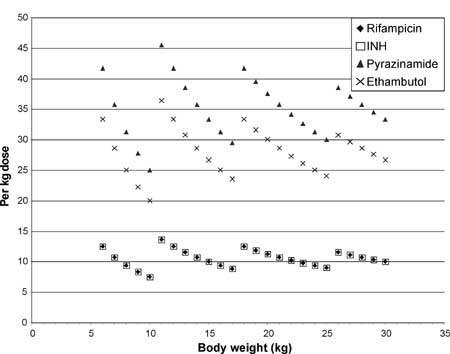
Introduction The Revised National Tuberculosis Control Program (RNTCP) has initiated provision of patient-wise boxes (PWBs) for antituberculosis therapy of children in 4 different weight bands (6-10 kg; 11-17 kg; 18-25 kg; 26-30 kg)(1). These medications are administered thrice weekly. Appropriate dosing of the drugs is necessary for getting good therapeutic response. When weight band based dosing is planned, it is important to ensure that all children receive adequate doses while taking care to avoid underdosing. Therefore, we evaluated the dose of individual drugs delivered by this approach to children of varying weights and discuss the concerns regarding the current protocol. Methods We used the protocol recommended by the RNTCP(1) for the 4 weight bands (6-10 kg; 11-17 kg; 18-25 kg; 26-30 kg) and evaluated the doses of individual drugs delivered by this approach using the Microsoft Excel spreadsheet. We calculated per kg drug delivered for each body weight and analyzed the same. We compared the dosing (RNTCP per kg dosing guidelines) with the doses recommended by the American Thoracic Society (ATS)(2), the British Thoracic Society (BTS)(3) and the WHO(4) for intermittent therapy in children with tuberculosis. Results Table I shows the doses for various weight bands (administered thrice weekly) in RNTCP schedule. Table II shows the doses recommended for (thrice weekly) intermittent therapy by various guidelines. Fig.1 shows the dose per kg of each of the drugs delivered at different body weights. It is evident that there is underdosing of rifampicin, INH, ethambutol and pyrazinamide for many of the weight categories, by RNTCP as well as the ATS, BTS and WHO guidelines for dosages of respective drugs. Table I Pediatric Doses in Different Weight Bands as Recommended by RNTCP(1)
ETH: Ethambutol; INH: Isoniazide Table II Recommended Doses (mg/kg) for Thrice Weekly Antituberculosis Regimen
Influence of change in body weight with treatment on the per kg dose of the drugs The PWBs are fixed and are not changed in the course of treatment. A child who is at the upper end of a weight band and gains weight with treatment will be underdosed even more if the PWB is not changed. Formulations The available tablets are not dispersible and it will be difficult to administer the tablets to young children particularly infants. Discussion On evaluating the dosing of various drugs as per recommendations of RNTCP, we identified three major concerns: underdosing of individual drugs; lack of provision to modify doses when child gains weight and moves to another weight band; and, inappropriate formulations, particularly for infants. Underdosing carries a significant risk of combined rates of failure during therapy plus relapse after therapy exceeding 5% and, risk of acquired drug resistance (>1%) even in patients on supervised therapy(5). The postantibiotic effect, the basis of successful intermittent therapy(6), achieved with lower peak serum levels may be less than desirable. We now review the literature to assess the minimum acceptable dose for each of the 4 antitubercular drugs. Rifampicin: A key USPHS trial demonstrated that doses of less than 9 mg/kg may be suboptimal(7). Subsequent trials have established the efficacy of a dose of 10 mg/kg/day of rifampicin in 6 and/or 9 month regimens (for both daily and intermittent therapy)(8). In areas with high prevalence of primary resistance to INH, this would effectively result in monotherapy with rifampicin at a suboptimal dose increasing the risk of development of MDR-TB especially in the continuation phase(9). Isoniazid: The recommended daily dose of INH in children is 10-20 mg/kg(10) with higher doses in tuberculous meningitis. This would achieve peak serum concentrations of 5 µg/mL. INH resistant M. tuberculosis strains contain katG gene mutations (50-80%) which confers high levels of resistance (MIC=5-10 µg/mL)(11). Giving suboptimal doses could have a significant risk of selecting mycobacteria with higher levels of resistance (MIC >5 µg/mL) to persist in the child and multiply, especially in the continuation phase leading to more failure rates. It is well accepted that the dose of INH has to be higher when given thrice weekly than when given daily(2). Ethambutol: It has been found that peak levels correlate with dose (i.e. 15 mg/kg/ dose ®2-4 µg/mL; 25mg/kg/dose ® 4-6 µg/mL)(12). The MIC of ethambutol for M. tuberculosis ranges from 2-4 µg/mL(13). The MBC range from 4-60 µg/mL(13). Thus, it is proposed that early antimycobacterial activity is often bacteriostatic rather than bactericidal. With doses ranging from 20-36 mg/kg that will be delivered according to the RNTCP schedule, the peak levels achieved would be in the bacteriostatic range only. It has been found that addition of ethambutol to HRS regimen did not increase the rate of 2-month negative cultures, a marker for relapse rate(14). Pyrazinamide: Its recommended dosage in intermittent therapy is 50- 75 mg/kg/dose(2) which would achieve peak plasma concentrations of 50-80 µg/mL (MIC of susceptible Mycobacteria ranging from £100 to 300 µg/mL)(15). However, the effect of underdosing of pyrazinamide on emergence of drug resistant TB has not been well documented. We conclude that the current dosing strategy used in RNTCP needs modification to prevent the significant risk of underdosing, undertreatment, and emergence of MDR- TB. Acknowledgment The authors thank Dr Yogesh Jain for reading the manuscript and providing critical comments. Contributors: RL will act as guarantor for the study. Funding: None. Competing interests: None stated.
nd Edition. Geneva: WHO/HTM/TB/2004.329. p. 112. 5. Vernon AA. Rifamycin antibiotics, with a focus on newer agents. In: Rom WN, Garay SM (Eds). Tuberculosis. 2 nd Edition. Philadelphia: Lippincott Williams & Wilkins; 2004. p. 759-771.6. Dickinson JM, Mitchison DA. In vitro studies on the choice of drugs for intermittent chemotherapy of tuberculosis. Tubercle 1966; 47: 370-380. 7. Long MW, Snider DE Jr, Farer LS. U.S. Public Health Service Cooperative trial of three rifampin-isoniazid regimens in treatment of pulmonary tuberculosis. Am Rev Respir Dis 1979; 119: 879-894. 8. Fox W, Ellard GA, Mitchison DA. Studies on the treatment of tuberculosis undertaken by the British Medical Research Council tuberculosis units, 1946-1986, with relevant subsequent publications. Int J Tuberc Lung Dis 1999; 3: S231-279. 9. Mahmoudi A, Iseman MD. Pitfalls in the care of patients with tuberculosis. Common errors and their association with the acquisition of drug resistance. JAMA 1993; 270: 65-68. 10. Kucers A. Isoniazid. In: Kucers A, Crowe SM, Grayson ML, et al. The Use of Antibiotics: A Clinical Review of Antibacterial, Antifungal and Antiviral Drugs. 5th ed. Boston: Butterworth-Heinemann; 1997. p. 1179-1210. 11. Abate G, Hoffner SE, Thomsen VO, Miorner H. Characterization of isoniazid-resistant strains of Mycobacterium tuberculosis on the basis of phenotypic properties and mutations in katG. Eur J Clin Microbiol Infect Dis 2001; 20: 329-333. 12. Lewis ML. Antibacterial agents: ethambutol. In: Yu VL, Merigan TC, Barriere SL, eds. Antimicrobial Therapy and Vaccines. Baltimore: Williams & Wilkins; 1999. p. 643-650. 13. Heifets LB, Iseman MD, Lindholm-Levy PJ. Ethambutol MICs and MBCs for Mycobacterium avium complex and Mycobacterium tuber-culosis. Antimicrob Agents Chemother 1986; 30: 927-932. 14. Hong Kong Chest Service/British Medical Research Council. Controlled trial of 6-month and 8-month regimens in the treatment of pulmonary tuberculosis:the results up to 24 months. Tubercle 1979; 60: 201-210. 15. Chan ED, Chatterjee D, Iseman MD, Heifets LB. Pyrazinamide, ethambutol, ethionamide, and aminoglycosides. In, Rom WN, Garay SM (Eds). Tuberculosis. 2nd Edition. Philadelphia: Lippincott Williams & Wilkins. 2004. p. 773-789. |
![]()