|
|
Short Communications Indian Pediatrics 2008; 45:-839-851 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Pyloric Atresia Associated with Epidermolysis Bullosa |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Alireza Alam Sahebpor, Vajihe Ghafari and Leila Shokohi From the Department of Pediatric Surgery, Mazandaran University of Medical Science, Sari, Iran. Correspondence to: Dr. Alireza Alam Sahebpor,
Department of Pediatric Surgery, Booali Sina Hospital, Manuscript received: January 18, 2007; Initial review
completed: January 24, 2007; Abstract
Introduction Pyloric atresia (PA) is a rare malformation which is estimated to be responsible for less than 1% of gastrointestinal atresia with an incidence of 1 in 100,000 live births(1). Epidermal bullosa (EB) is a group of hereditary disorders of skin where the primary cause is the formation of blisters following minor trauma. It is categorized as EB simplex (EBS), junctional EB (JEB), and dystrophic EB (DEB). Evidence suggests that PA-EB association is a distinct entity, referred to as the PA-EB syndrome(2). Hitherto, the association of PA-EB was thought to be fatal because of septicemia, electrolyte imbalance and protein loss seen in EB. It was even recommended in the past that surgical treatment be withheld in these patients. We report good results with surgery in these children and better survival rate. Methods This study was conducted in the pediatric surgical units of Boo-Ali hospital in Sari, Iran from 2003 to 2005. We had 5 patients with PA associated with JEB. Biopsy of bullae was done in all patients for confirmation of diagnosis. All children were subjected to surgery. The details are shown in Table I. Table I Details of Cases of Pyloric Atresia - Epidermolysis Bullosa
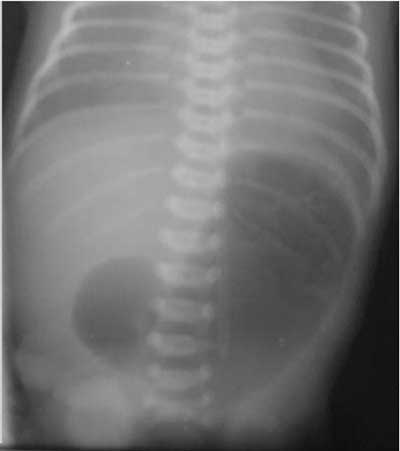
* Not available Results There were 4 boys and one girl. Mean age of presentation was 8.4 days (3 to 15 days). There were multiple bullous skin lesions over the extremities in all of the patients (Fig.1). An abdominal X-ray in first patient showed distended stomach with no distal gas (Fig.2). All underwent laparatomy after stabilization. Four neonates with type 2 PA underwent gastroduodenostomy, and the one patient with type 1 PA had excision of membrane and pyloroplasty. By 6 to 36 months follow-up (mean 21.6 months), all 4 surviving infants are doing well. One child died on 12th postoperative day.
Discussion The earliest description of PA is credited to Caleder in 1749(3), and Swinbure and Kohler first described the association of PA and EB in 1968(4,5). The typical presentation of PA is non bilious vomiting soon after birth without abdominal distention. The diagnosis is made easily on plain abdominal X-ray, which shows a single gas field bubble representing the distended stomach with no distal gas. Antenatal ultrasound may show polyhydramios and dilated stomach(6). Prematurity and polyhydramnios are found in most of these patients as in our first and third patients. The surgical treatment of pyloric atresia depends on the type of atresia. In type 1 PA, membrane is excised and Heieke-Mikulicz pyloroplasty is performed(7,8). For type 2 atresia the surgical treatment is excision of atretic segment and gasterodeodenustomy(7,9). For type 3 also the surgical treatment is gastroduodenostomy(10). Gastrojejunostomy is better avoided because of 59% failure and 55% mortality(11). Epidermolysis bullosa presents with blisters, crusted erosions and scar formation. Of the 3 types of EB, JEB is mostly associated with PA(12,13). Whereas the surgical management for PA is straightforward, septicemia, electrolyte imbalance, protein loss and failure to thrive complicate the severe exudative skin lesions, often leading to death. This has led to recommendation that surgical treatment be withheld in patients with PA-EB. Four of our cases were stable before operation, and tolerated it well. They are all well on follow-up visits. Follow up was from 6 to 36 months. One case was not in good condition and died of sepsis after operation. Postoperatively, all 4 survived patients tolerated feeding well and went home with no problem. Another series by Hayashi, et al.(11) also recommends that stable infants with PA-EB should be treated surgically. Samad, et al.(2) reported 3 cases of PA-EB; only one survived. They concluded that although the prognosis is poor in this condition, surgery should not be withheld on assumption of high mortality(2). We also suggest surgical treatment for neonates with PA-EB who are stable. Contributors: All authors contributed to study design, literature review and drafting of the manuscript. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
![]()