|
|
Research Papers Indian Pediatrics 2008; 45:819-823 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Immunogenicity and Safety of an Indigenously Developed DTPw-Hepatitis B Combination Vaccine in Indian Infants |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Raju Shah*, MB Raghu**, A Shivananda***, S
Mangayarkarasi#, I Rao+, R Rao++, P Bhusari++, From the *Department of Pediatrics, Shardaben General Hospital & Smt NHL Municipal Medical College, Ahmedabad; ** Department of Pediatrics, Sri Ramchandra Medical College Hospital, Chennai; ***Department of Pediatrics, Indira Gandhi Institute of Child Health and Hospital, Bangalore; #Department of Pediatrics, Institute of Child Health and Hospital for Children, Chennai; +Department of Pediatrics, Institute of Child Health, Niloufer Hospital, Hyderabad; and ++Clinical Research Division, Shantha Biotechnics Ltd., Hyderabad, India.*Correspondence to: Dr. Raju C Shah, Consultant
Pediatrician & Neonatologist, Ankur Institute of Child Health, Manuscript received: January 2, 2007; Initial review
completed: August 8, 2007;
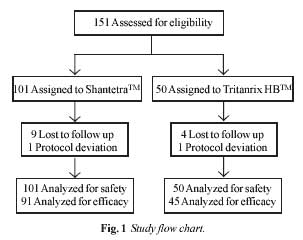
Introduction Diphtheria, tetanus and whooping cough (pertussis) are common infectious diseases prevalent in developing countries. An estimated 350 million individuals are chronic carriers of the Hepatitis B virus worldwide(1). Separate vaccines are presently being used for prevention of these diseases (DTP and hepatitis B vaccines). Combination of hepatitis B component with DTPw vaccine, which is a part of EPI schedule, offers some advantages; both are adsorbed products, are administered in multiple doses in the first year of life and the schedules of hepatitis B vaccine are compatible with DTPw schedules. Studies have shown that the hepatitis B component does not interfere with the immune response to the DTPw component of the quadrivalent vaccine and vice versa(2,3). We conducted this trial to compare the safety and immune response of a tetravalent DTPwH vaccine (ShantetraTM, Shantha Biotechnics Limited, India) with Tritanrix HBTM vaccine (GSK Biologicals, Rixensart, Belgium). Methods The present trial was conducted at five tertiary care referral centers viz: Ankur Institute of Child health (Ahmedabad), Sri Ramchandra Medical College Hospital (Chennai), Indira Gandhi Institute of Child Health (Bangalore), Institute of Child Health and Hospital for Children(Chennai), and Institute of Child Health, Niloufer Hospital (Hyderabad). The subjects were recruited and followed up on outpatient basis. A single protocol, approved by ethics committee at each center, was used in the study to ensure uniformity. Subjects: Healthy infants 6 to 8 weeks of age and born to mothers negative for hepatitis B surface antigen (HBsAg) during pregnancy, were recruited. Subjects having evidence of fever, or history of hematological, hepatic, renal, cardiac, respiratory, or neurological disease and, immunodeficiency at the time of vaccination were excluded. The subjects had also not received any immunoglobulins, blood products or any other concurrent vaccine with the exception of OPV and BCG. Study design: The study was approved by the local Institutional Ethics Committees at all the sites. After written informed consent was obtained from the parent or the legal guardian at the study centers, the infants were screened and assessed for selection criteria. The infants eligible for selection were randomized to receive either ShantetraTM or Tritanrix HBTM, in a ratio of 2:1 at all the centers. Randomization was carried out using the PROC PLAN. Two venous blood samples, pre vaccination and 4-6 weeks post third dose, of 1.5 mL each were obtained from each subject for determination of DTP and anti-HBsAg antibodies. All vaccine doses were administered intramuscularly in the anterolateral thigh region. The first dose was administered at approximately 6-8 weeks of age while the second and third doses were administered at 10-12 and 14-16 weeks, respectively. The identity of the vaccine was concealed from the parent or the legal guardian of the subjects. For the first 30-60 minutes after each dose, the infants were observed directly for any adverse reaction. The parents or guardian were also given diary cards on which to record observations and were asked to return the same on the following visit. The diary cards were designed to record information on specific local, systemic and other unsolicited reactions. Vaccines: Each 0.5 mL dose of ShantetraTM, the DTPw-HB tetravalent combination vaccine used in this trial, contained diphtheria toxoid 25 Lf, tetanus toxoid 5 Lf, 15 OU of inactivated whole-cell B. pertussis and 10 µg of HB surface antigen, with 0.025 mg of thiomersol as preservative and 0.625 mg of aluminum salts as adjuvant. The comparator vaccine Tritanrix HBTM, contained diphtheria toxoid 30 IU, tetanus toxoid 60 IU, 4 IU of B. pertussis and 10 mcg of HB surface antigen, with 0.025 mg of thiomersol as preservative and 0.63 mg of aluminum salts as adjuvant. Serological analysis: Serological analysis for estimation of antibodies was carried out at a central laboratory. Anti-diphtheria and tetanus antibodies were measured using IgG-ELISA from Virion-Serion Immunodiagnostica (GmbH, Germany), whereas pertussis antibodies were estimated using IgG-ELISA from NovaTec Immundiagnostica (GmbH, Dietzenbach, Germany). Anti-HBsAg antibodies were estimated by Abbott Diagnostics (AUSAB). Geometric Mean Titers (GMT) were calculated using the post-vaccination antibody levels. Upper and lower 95% confidence intervals were calculated for all GMTs. Percentage of subjects who had protective levels of anti-Hbs (³10 mIU/mL), anti-diphtheria antibodies (³0.1 IU/mL) and anti-tetanus antibodies (³0.1 IU/mL) was also determined. Response to pertussis component was defined as a post vaccination antibody levels ³11 NTU/mL (as per assay cut off) for initially seronegative subjects. In case of initially seropositive subjects, a post vaccination titer more than or equal to the pre-vaccination titer was considered to be protective. Every subject randomized in the study was analyzed for safety, except if he/ she did not receive any injection of the study vaccines or if no post randomization data was collected for this subject. As per protocol analysis, subjects who satisfied the inclusion/ exclusion criteria and properly followed the protocol were analysed for efficacy. Following non-compliant subjects were excluded from the sample: subjects included without meeting at least one inclusion criterion; subjects included despite meeting at least one exclusion criterion; subjects found non compliant with the blood sampling schedule; subjects vaccinated with the wrong vaccine (non compliance with the randomization code); and, subjects excluded from the intention-to-treat analysis. All statistical analysis were carried out using SAS software. Results Overall, 151 babies were recruited at five centers to recruit 101 in the ShantetraTM group and 50 subjects in the Tritanrix HB group. Of these subjects 136 were evaluable for immunogenicity using per protocol analysis and all 151 were available for safety using intention-to-treat analysis (Fig. 1). Overall fifteen babies were excluded from immunogenicity analysis, of which 10 were in the Shantetra group and 5 were in the Tritanrix HB group. 13 out of 15 were lost to follow-up while there were 2 protocol violations (1 in each group). Hence efficacy analysis was done in 91 infants in the Shantetra group and 45 in the Tritanrix HB group. The demographic profile of the subjects recruited is shown in Table I.
TABLE I Profile of Recruited Subjects
The immune responses to the vaccine components are represented in Table II. Overall, 98.9% of the vaccinees were protected against hepatitis B, diphtheria and tetanus in the Shantetra group while 95.5 % vaccinees responded in the comparator group. It was observed that 61 and 40 subjects in the Shantetra and Tritanrix HB groups, respectively had the pre-vaccination titers ³0.1 IU/mL (protective levels) for tetanus toxoid; this may be related to the vaccination of the mothers with two doses of tetanus toxoid during gestation leading to passive transfer of antibodies in the neonates. TABLE II Seroprotection with ShantetraTM and Tritanrix HBTM Vaccine
A total of 26 (19.1%) subjects (18 and 8 in Shantetra and Tritanrix HB groups, respectively) received the hepatitis B vaccine at birth. No significant difference in seroconversion rates (100% vs 98.63%, P=0.34 and 100% vs 91.9%, P=0.41) was observed among subjects who received the hepatitis B vaccine at birth, and those who did not in the Shantetra and Tritanrix HB groups, respectively. Two (2.1%) infants in Shantetra group and 3 (6.7%) in the Tritanrix HB group had protective levels of (³ 10 mIU/mL) anti-HBsAg antibodies prior to vaccination. All five had received the first dose of vaccine at birth. The GMT in the study group was significantly higher than the comparator (473.3 vs. 265.7, P<0.05). It was also observed that 11(13.5%) subjects in the Shantetra group and 6 (14.6%) in the Tritanrix HB group had pre-vaccination antibody titers ³11 NTU/mL (protective levels) for B. pertussis. In 10 (12.3%) subjects in Shantetra group and 4 (9.7%) in the Tritanrix HB, group the post-vaccination titers were less than the pre-vaccination values, but all these infants had protective levels of ³11 NTU/mL. Overall 81(89 %) of 91 infants in the Shantetra group and 41 (91.1%) of 45 in comparator group seroconverted after vaccination. The local and systemic reactions after vaccine doses are represented in Table III. Fever following vaccination was mild in nature, subsided within 6-12 hours and did not recur. There were no serious adverse events reported during the study. TABLE III Local and Systemic Side effects observed with ShantetraTM and Tritanrix HBTM
Figures in parentheses indicate percentages Discussion This randomized, single blind, comparative multicentric trial evaluated indigenous DTPw-HBV combination vaccine (Shantetra). The vaccine demonstrated efficacy and safety in terms of the immune response to all antigens and adverse event profile, when administered according to a 6-10-14 week EPI schedule. Shantetra induced strong immune response to all vaccine components; 98.9% of the vaccinees were protected against hepatitis B, diphtheria and tetanus infections in the Shantetra group while 95.5% vaccinees responded in the comparator group. The GMTs in the Shantetra group for anti HBsAg antibodies were significantly higher in comparison to Tritanrix HB (P<0.05). The GMTs for rest of the antigens were comparable in both the groups. This fulfills the WHO recommendation that there should be at least 95% protection against hepatitis B infection after three doses of the vaccine. Overall 89% and 91.1% of subjects in the study and Tritanrix HB groups, respectively responded to pertussis component. The reactogenicity and immunogenicity profile of the candidate vaccine was similar to that of Tritanrix HB and no serious adverse events were reported in either group. Combining the HB component with DTP vaccine did not have any effect on the immunogenicity of the HB component. The frequencies of the local and general symptoms are similar to what have been previously reported in other studies. The occurrence of reactions associated with DTP are mostly caused by the whole cell pertussis component. Unlike previously reported studies, both the groups receiving whole cell and acellular pertussis vaccine had similar frequencies of local and systemic reactions(4). The reactions seen with the candidate vaccine are similar in nature and frequency to those observed with the comparator and previously reported(2,3). In the present study, a decrease in incidence of adverse events in vacinees following successive doses of the vaccine in both the groups has been observed. This is in agreement with the meta-analysis reported in a Cochrane Collaboration review of the adverse event profiles of whole cell and acellular pertussis vaccines(5). There was a fall in the incidence of swelling, redness, pain, irritability, fever and prolonged crying in both study groups after successive doses of vaccines. The major limitation of this study is that the sample size is not adequate enough to elicit any rare or previously unreported adverse events. The same can be studied by conducting large safety studies for the vaccine. Shantetra, the candidate DTPw-HB combination vaccine has shown satisfactory results with regards to safety and immunogenicity when administered to healthy infants in the 6, 10 and 14 week schedule. Contributors: RS, MBR, AS, SM and IR were the principal investigators for the study and provided day to day supervision of patient-recruitment and follow-up, and provided inputs towards the finalization of the manuscript. RR, PB CAJ and RR were involved in conceiving and designing the study and the protocol, and were also involved in the development and critical review of the manuscript. The final manuscript was approved by all the authors. RR will act as the guarantor of this paper. Funding: Shantha Biotechnics Limited, Hyderabad, India. Competing interests: One of the vaccines used in this study (Shantetra TM) is being commercially marketed by Shantha Biotechnics Limited. Dr Raman Rao, P Bhusari, CA Joseph and Dr R Reddy are employees of Shantha Biotechnics Limited.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()