|
|
Review Article Indian Pediatrics 2007;44:785-787 |
||
|
Atypical Relapsing Course of Kawasaki Disease with Hemorrhagic Serous Effusions and Hepatic Dysfunction |
||
|
K.E. Elizabeth
From the Department of Pediatrics and Division of Pediatric Cardiology, SAT Hospital. Govt. Medical College, Thiruvananthapuram, Kerala, India 695 011. Correspondence to: Elizabeth K E, Department of Pediatrics, SAT Hospital. Govt. Medical College, Thiruvananthapuram, Kerala, India 695 011. E-mail: elizake@hotmail.com Manuscript received: December 4, 2006; Initial review completed:
February 8, 2007;
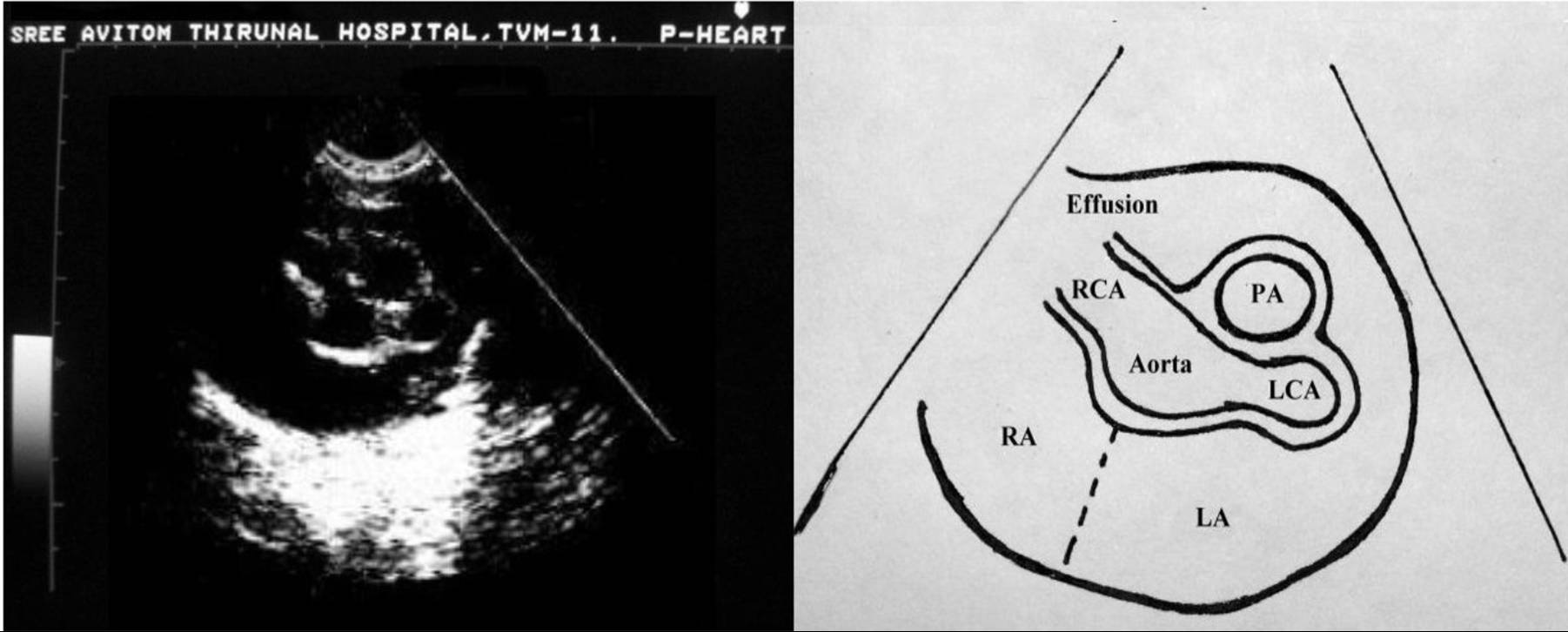
Atypical Kawasaki disease, Hemorrhagic pleural effusion. Kawasaki disease (KD) is a multisystem disease of childhood with vasculitis involving medium sized arteries(1). Atypical KD is diagnosed with fever and fewer than four of the five clinical criteria(2). Early diagnosis and prompt treatment with aspirin and intravenous immunoglobulin (IVIG) within the first 10 days of illness can reduce coronary artery lesions (CAL) and aneurysm, from 20% in untreated to 5%(3). KD has close resemblance to staphylococcal and streptococcal infections, measles, infectious mononucleosis and drug hypersensitivity syndromes,(1,2) that can also lead to peeling of skin during convalescence. Cardiac, renal, pulmonary and neurological manifestations are known in this condition(4,5). Lung involvement with cough, coryza, pulmonary infiltration, pleural effusion, arteritis, interstitial pneumonia, interstitial pneumonitis with organizing pneumonia (IPOP) and fibrosis are also described(6,7). Hemorrhagic pleural effusion is a rare manifestation in KD(8). We report an atypical case of KD with a relapsing course and subsequent development of hemorrhagic serous effusions, CAL, hepatic dysfunction and rash with peeling in spite of administration of IVIG and aspirin during the first admission. Case Report A 3-year-old girl was admitted with fever of 3 weeks duration and gum bleeding. The child was very irritable and had a temperature of 39.5ºC, heart rate 110/minute, respiratory rate 56/minute and blood pressure of 110/60 mm Hg. She had left sided anterior cervical lymph nodes measuring about 1.5×2 cm in size. There was erythema and erosion in the oral cavity and bilateral pitting pedal edema. There was no conjunctivitis, arthritis or rash. Initially hemoglobin was 10.2 g/dL, total WBC count 12,800/cumm with 74% neurtrophils, 25% lymphocytes and 1% eosinophils. Platelet count was 550000/cumm, ESR 86 mm/1st hr and elevated C Reactive Protein (CRP) 7.7 mg/dL (normal <6 mg/dL). Coagulation profile, serum electrolytes, blood urea, creatinine, lipid profile, bilirubin, liver enzymes and urine analysis were normal. Mantoux skin test was negative. Anti Steptolysin O (ASO) titre, Widal test, anti nuclear antibody (ANA) and rheumatoid arthritis (RA) factor were negative. Blood culture was sterile. A provisional diagnosis of atypical KD was considered based on fever more than 5 days duration, mucosal lesions, unilateral cervical lymphadenopathy and pedal edema satisfying 3 out of 5 criteria. Echocardiogram revealed a normal heart with normal coronaries. On admission, the child was started on crystalline penicillin and cloxacillin. Considering KD, IVIG 2 g/kg in two divided doses, aspirin in anti-inflammatory dose of 100 mg/kg/day and other supportive measures were given. Child improved and was discharged on the 7th day on aspirin. ESR decreased to 25 mm, platelet count became 1,50,000/ cu mm and CRP was negative (4 mg/dL). Aspirin was stepped down to antiplatelet dose of 5 mg/kg/day after two weeks of therapy. The child was readmitted after one month with high fever of 3 days duration and edema of face and feet. Temperature was 40ºC, heart rate 120/minute, respiratory rate 46/minute and blood pressure 100/70 mm Hg. She had bilateral pitting pedal edema, icterus, abdominal distension and hepatomegaly. Investigations revealed the following; hemoglobin 8.6 g/dL, total WBC count 5500/cumm with 58% neurtrophils and 32% lymphocytes, platelet count 80,000/cumm, ESR 25 mm/hr, elevated CRP (8.7 mg/dL) and RBS 75 mg/dL. Renal function tests were normal, but liver function tests were abnormal with serum bilirubin 2.1 mg/dL which increased to 5.4 mg after admission, SGOT 2945 U/L, SGPT 1755 U/L and alkaline phosphatase 350 U/L. Prothrombin time was 33 sec (control 12.3, INR 2.82). APTT was >100 sec. ASO titer, ANA, Anti Ds DNA, RA factor and CPK were negative. Viral markers including dengue IgM, HBs Ag antigen and anti HCV and anti HAV antibodies (ELISA) and leptospira IgM antibody were negative. HIV ELISA was negative. Repeat blood culture was also sterile. Serological tests may not be reliable immediately after IVIG administration, but this child was readmitted one month after IVIG administration. Aspirin was stopped and she was managed as hepatic failure with supportive measures including ampicillin, fresh frozen plasma (FFP) and parenteral vitamin K. Chest X-ray on the day of admission showed prominent broncho-vascular markings. Echocardiogram done on the next day showed significant bilateral coronary dilatation with pericardial effusion. Right sided pleural effusion was also noted. Figure 1 depicts the Echocardiogram findings. Ultrasound scan of the abdomen showed hepatomegaly, ascites and right sided pleural effusion.
Child developed severe respiratory distress the next day; repeat chest X-ray showed massive right pleural effusion. An intercostal tube was inserted, which drained about 500 mL of hemorrhagic fluid. It showed plenty of RBCs and occasional lymphocytes and neutrophils, sugar was 85 mg/dL, protein 1.1 g/dL and abnormally high LDH 10031 U/L. Pleural fluid to serum LDH was >0.6 (serum LDH normal 150-500 U/L). Gram stain and AFB stain were negative. Child was given FFP and fresh blood transfusion in view of the bleeding manifestation. IVIG 2 g/kg in two divided doses was repeated on 3rd and 4th day of admission as the child had evidence of recurrence of KD with CAL. The fever and irritability persisted. She had increasing coronary artery dilation noticed on repeat echo-cardiograph done on 5th day. Hence, she was also given pulse methylprednisolone in a dose of 30 mg/kg/day for 3 days. Repeat laboratory investigations showed prothrombin time of 18.4 seconds (control 12.3, INR 1.53), APTT 40.6 seconds (control 32), SGOT 562 U/L, SGPT 540 U/L. Repeat ESR value was 45 mm /1st hr. CRP was negative (4 mg/dL) and platelet count became 300000/cu mm. She gradually improved over the next 2 weeks and was discharged on low dose aspirin. Aspirin was restarted in antiplatelet dose before discharge. Three weeks later, she was readmitted with fever, itching and maculopapular rash of 3 days duration. Drug rash/ erythema multiforme was suspected and she was reinvestigated. Repeat echocardiogram showed no further dilatation of the coronaries. Hemoglobin was 8.8 g/dL, total WBC Count 11000/ cumm, P 74%, L 25%, E 1%, platelet count 2,40,000/ cu mm , ESR 113 /1st hr and CRP was negative (2.5 mg/dL). Renal function, serum bilirubin and coagulation profile were normal. Liver enzymes were elevated, SGOT 113 IU/L, SGPT 102 IU/L. She responded to topical calamine lotion and antihistaminics and was discharged after one week of observation. She developed peeling of skin later on. The rashes suggest relapse of KD due to high ESR and subsequent peeling of skin. The child is currently on antiplatelet dose of aspirin and is asymptomatic for the last one year. Discussion This child presented initially with atypical KD after 3 weeks of illness leading to delayed administration of IVIG and aspirin. The other unique features were the following: (i) coronary artery dilatation developing 1 month later in spite of IVIG and aspirin therapy; (ii) hemorrhagic pleural effusion with pericardial effusion and ascites presenting as polyserositis syndrome during relapse; (iii) hepatic dysfunction with altered coagulation profile and thrombocytopenia during relapse, (iv) fever, rashes with subsequent peeling and relapsing high ESR appearing 2 months later; and (v) relapse requiring re-treatment with IVIG and pulse methylprednisolone. Macrophage activation syndrome with hepatic dysfunction can occur in KD, but it is a fatal condition with low ESR, pancytopenia, hepato-splenomegaly etc. But our patient did not have such features and she improved. Immunoglobulin resis-tant KD with polyserositis syndrome and cardiac tamponade that responded to methylprednisolone has been reported(9). Even though, hemorrhagic pleural effusion in KD has been reported in one case(8), liver dysfunction, thrombocytopenia and abnormal coagulation profile are not reported. Contributors: EKE: Consultant in charge, Conception, design and revision of manuscript, MZA: Cardiology consultant in charge and PKS; Involved in case management and acquisition of data. Funding: None. Competing interests: None.
| ||
|
References | ||
|
|
![]()