|
|
Short Communication Indian Pediatrics 2007; 44:771-773 |
||||
|
Growth Pattern and Final Height in 21-Hydroxylase Deficiency |
||||
|
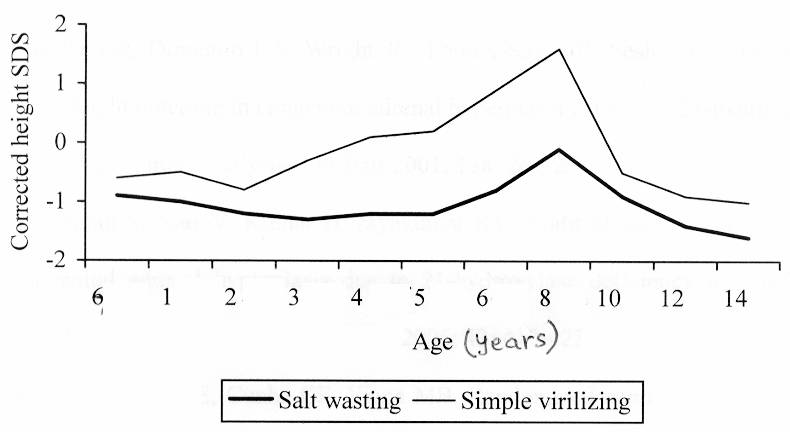
Growth pattern and final height were evaluated in 47 children with 21-hydroxylase deficiency to identify factors influencing growth. The subjects were followed-up from the age of 0.6 ± 1.2 years for 8.8 ± 3.9 years. Final height SDS was significantly below target height SDS (–2.5 ± 1.4 versus –1.0 ± 1.0, P <0.001). Laboratory monitoring and type of disease (salt-wasting or simple virilizing) significantly influenced age-specific height SDS. Age at treatment, frequency of laboratory monitoring and dose of glucocorticoid during infancy influenced final height on univariate analysis; the effect was not sustained on multivariate analysis. Our study emphasizes the need for regular laboratory monitoring and lower glucocorticoid dose during infancy in 21-hydroxylase deficiency. Key words: 21-hydroxylase deficiency, Congenital adrenal hyperplasia, Glucocorticoids, Growth. Despite significant advances in the management of 21-hydroxylase deficiency (21-OHD), growth compromise is a major cause of concern(1). The outcome is compromised in resource-poor countries with inadequate laboratory facilities and uneven supply of medicines(2). Delayed treatment, use of synthetic glucocorticoid preparations and higher glucocorticoid doses are associated with poor height outcome in 21-OHD(3,4). There is a paucity of data about factors influencing growth 21-OHD in resource-poor countries. We performed this study to evaluate factors influencing growth in 21-OHD. Subjects and Methods We reviewed case records of children with 21-OHD followed-up in the Pediatric Endocrinology Clinic for more than five years. 21-OHD was diagnosed using the standard criteria(5). Hydro-cortisone was the recommended glucocorticoid preparation; prednisolone was used by patients who could not afford hydrocortisone. For estimating glucocorticoid doses, 1 mg of prednisolone was considered equivalent to 4 mg of hydrocortisone(6). Estimation of 17-hydroxyprogesterone (17OHP) and dehydroepiandro-sterone (DHEA) levels was advised prior to each three-monthly visit. The glucocorticoid dose was adjusted to achieve a growth velocity between 25th and 75th percentiles for age and target 17OHP (100-1000 ng/dL) and DHEA levels (50-100 ng/dL). Clinical parameters alone were considered for adjusting glucocorticoid dose in children who could not afford these investigations. Mineralocorticoid dose was modi-fied according to blood pressure and serum electrolytes. Target height (TH) was calculated using standard formula. Patients were considered to have attained final height when they had a growth velocity less than 0.5 cm/year and a bone age more than of 15 years(7). Height data was expressed as standard deviation score (SDS) using NCHS data(8). Corrected height SDS was calculated by deducting target height SDS from height SDS. Factors influencing growth pattern and FH were evaluated using repeated measure and linear regression analysis respectively. Values were expressed as mean ± standard deviation unless specified. P value less than 0.05 was considered significant. Results Forty-seven patients, 30 with salt-wasting (13 girls) and 17 with simple virilizing form (15 girls) were included in the study. Patients were followed from the age of 0.6 ± 1.2 years for 8.8 ± 3.9 years till the age of 9.4 ± 3.9 years. Hydrocortisone was used by 40 patients; two boys with salt-wasting form and five girls with simple virilizing form had received prednisolone. The mean glucocorticoid dose was higher in children the salt-wasting compared to those with simple virilizing form throughout on repeated measure analysis (P <0.001). Growth and biochemical parameters were considered while adjusting glucocorticoids in 26 subjects with regular laboratory monitoring; growth parameters alone were used in the remaining 21 patients who could not afford blood tests. Growth pattern is presented in Fig.1. The greatest growth deceleration occurred during infancy and puberty. Repeated measure analysis revealed positive effect of laboratory monitoring (0.91; 95% CI 0.41-1.41; P <0.001) and simple virilizing form (1.07; 95% CI 0.54 -1.61; P <0.001) on age-specific height SDS. Growth pattern was not influenced by gender, steroid formulation, glucocorticoid dose or age at diagnosis.
Of the 20 subjects who had achieved final height at last follow-up, 13 (65%) had final height SDS in the target height range. Final height SDS was however significantly below target height SDS (–2.5 ± 1.4 versus –1.0 1 : 1.0, P <0.001). Regular laboratory monitoring was associated with higher corrected final height SDS (–0.9 ± 1.2 versus –2.2 ± 1.3, P = 0.007). Early treatment, regular laboratory monitoring and lower glucocorticoid dose during infancy had positive impact on FH on univariate analysis. This was not sustained on multivariate analysis. Final height SDS was not influenced by disease form, gender or glucocorticoid preparation. Discussion Despite improvement in auxological outcome, compromised growth is an issue of concern in Indian children with 21-OHD. The height outcome in our study was worse compared to reports from developed countries(1-3). Laboratory monitoring emerged as an important factor influencing growth in this study. Adjustment of steroid dose based on a combination of growth and biochemical parameters resulted in better height outcome compared to that based on growth parameters alone. Thus growth parameters need to be combined with laboratory monitoring to achieve optimal growth. This is especially true during periods of rapid growth like infancy and puberty where growth deceleration is evident only after a significant loss of growth potential. The greatest growth deceleration in this study was observed during these two periods emphasizing the need for regular monitoring during these critical phases. The effect of laboratory monitoring on growth in our study may have been confounded by the likelihood of better socio-economic status and compliance in patients undergoing laboratory monitoring. Glucocorticoid excess is an important cause of growth retardation in 21-OHD. We observed age-dependent growth suppressing effects of gluco-corticoid dose in our patients. While glucocorticoid dose during infancy influenced final height SDS on univariate analysis; it had no effect on age-specific height SDS. These observations and the demons-tration of growth-suppressing effects of high glucocorticoid dose during infancy and puberty highlights the importance of using lower gluco-corticoid doses during these critical phases of growth(9). We did not observe any effect of the type of disease, age at treatment, gender and steroid formulation on growth. Steroid formulation has significant effect on growth due to substantially greater growth-suppressing effect of synthetic glucocorticoid preparations like prednisolone and dexamethasone compared to hydrocortisone. Despite recommendations for the use of hydro-cortisone in 21-OHD, prednisolone was used by some Indian children due to uneven supply of hydrocortisone. Increasing availability of hydro-cortisone has been shown to improve growth in Indian children with 21-OHD(10). Lack of effect of steroid formulation on growth in our study may be due to relatively small number of patients who received prednisolone (n = 7, 14.9%). The findings of our study emphasize the need for improvements in the management of 21-OHD with lower steroid doses during infancy and regular laboratory monitoring. Contributors credit: AB, MK and PSNM were involved in the management of patients. AB planned the study, collected data, performed statistical analysis and drafted the manuscript. MK was involved in planning of the study and reviewed the script. RMP was involved in statistical analysis. PSNM was involved in planning the study, critically reviewed the manuscript and would act as the guarantor of the study. Funding: None. Competing interests: None.
| ||||
|
References | ||||
|
|
![]()