|
|
Letters to the Editor Indian Pediatrics 2006; 43:920-922 |
|||||||
|
Chiari Malformation Type II with Vanishing Cerebellum |
|||||||
|
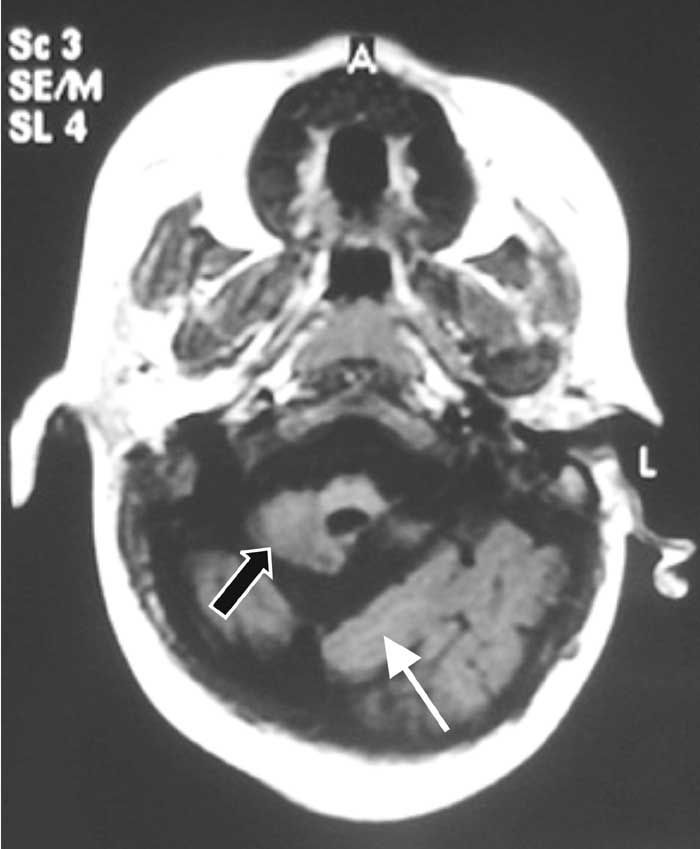
MR imaging revealed a small posterior fossa occupied by the occipital lobes and a profoundly small cerebellum (Fig 1). The tentorial incisura was heart-shaped. Sagittal sections demonstrated hypoplastic cord-like cerebellar tonsils herniating through the foramen magnum into the upper cervical canal and an elongated poorly-formed fourth ventricle (Fig. 2). Other findings were a small-sized pons with loss of normal pontine prominence, caudal elongation of the medulla and beaked tectal plate. The torcular hetero-phili was low-placed and supratentorial hydrocephalus was present. The massa inter-media was absent and the falx was hypoplastic with consequent interdigitations of gyri.
MR images of the lumbosacral spine revealed dysraphism and lumbar meningomyelocele with tethering of the cord. In 1891, Hans Chiari first described an anomaly encompassing elongated peg-like cerebellar tonsils displaced into the upper cervical canal through the foramen magnum to be later known as the Chiari type I malformation. Chiari type II anomaly includes herniation of the medulla, fourth ventricle and cerebellar vermis through the foramen magnum. Chiari III combines features of Chiari II with a high occipital or low cervical encephalocele. A fourth variety includes severe hypoplasia/aplasia in a diminutive posterior fossa. The Chiari II malformation is always associated with a meningomyelocele. This condition includes downward displacement of medulla, fourth ventricle and cerebellum into the cervical spinal canal, with concomitant elongated pons and fourth ventricle, probably due to a relatively small posterior fossa. These intracranial abnormalities are a result of incomplete closure of the neural tube, which prevents transient closure of the central canal that is essential for distension of the primitive ventricular system. The subsequent lack of the inductive effect of pressure and volume on the surrounding mesenchyme results in an abnormally shallow posterior fossa(1). Exceptionally, this transforaminal herniation results in ‘degeneration’ of cerebellar tissue, presenting as ‘the vanishing cerebellum in Chiari II malformation(2). The absence of a normal-sized posterior fossa precludes the diagnosis of cerebellar agenesis(3). N. Chidambaranathan,
|
![]()