|
|
Case Reports Indian Pediatrics 2006;43:905-907 |
||||
|
Recurrent Intracranial Hemorrhage in Brain Tumor |
||||
|
Sumana Datta (Kanjilal) From Department of Pediatric Medicine, Midnapore Medical College, Paschim Medinipur, West Bengal, India and Department of Pediatric Medicine, R.G. Kar Medical College, Kolkata, India.
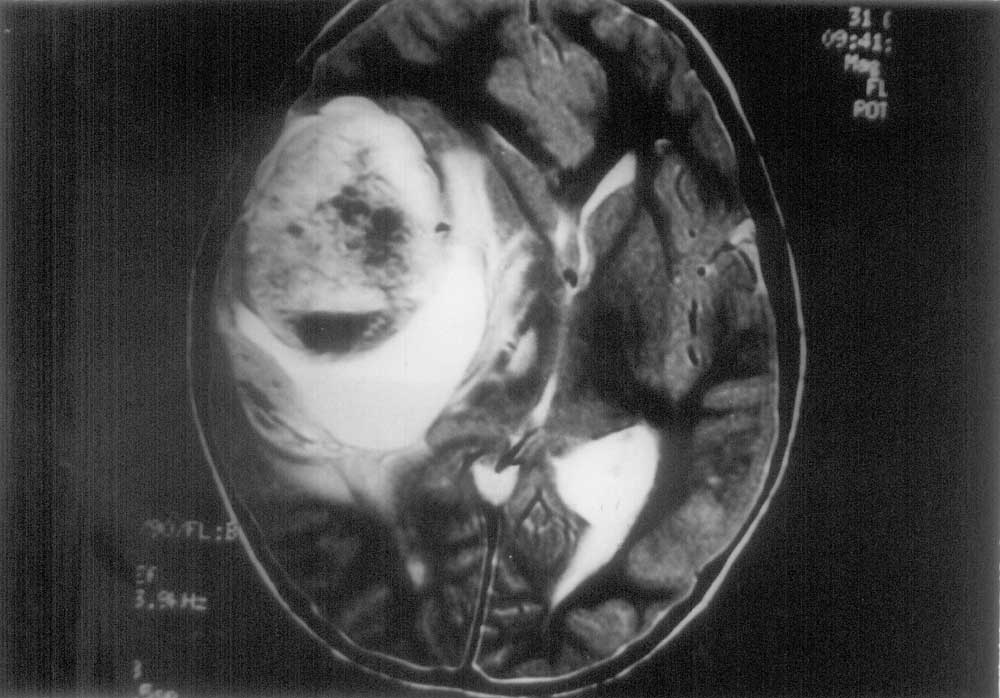
Recurrent intracranial hemorrhage with hemiparesis may be due to arteriovenous (AV) malformation, ruptured berry aneurysm, bleeding disorder or pheochromocytoma. Malignant neoplasm of brain such as glioblastoma multiforme may also cause recurrent intra-tumoral bleed resulting in hemiparesis in children. The rapidly growing tumor mass with bleed in it will ultimately cause mass effect. Case Report A seven-year-old male child was admitted with intense headache for the last four days, which was holocephalic, episodic and was specially aggravated at night. There was no history of vomiting, visual disturbances, convulsion or any other complaints. On examination, the child was drowsy, there was bradycardia (pulse rate-60/min, otherwise regular), mild hypertension (BP-128/88 mm of Hg). There was no other significant finding on general survey. Examination of central nervous system revealed bilateral papilledema. There was no cranial nerve palsy and focal neuro-logical deficit. Examination of other systems revealed no abnormality. After two days headache became continuous and the child gradually developed right-sided 3rd cranial nerve palsy with episodes of neck pain. Within next three days consciousness deteriorated and signs of tentorial herniation developed gradually. There was dilatation of left pupil followed by left sided hemiparesis. The child was admitted 6-months ago with generalized tonic-clonic convulsions. It was not associated with fever, vomiting or head injury. There was early papilledema with left sided hemiparesis. There was no evidence of bleeding disorder, skin changes, hypertension and no history of intake of anticoagulant drugs. Family history was not significant. Hemogram including coagulation profile, chest skiagram, USG abdomen and other investigations revealed no abnormality. CT scan and MRI brain showed right-sided temporo-parietal hematoma. The child recovered quickly within next 2-3 weeks without any residual weakness of limbs and repeat CT scan and MRI brain after 4 weeks revealed resolving hematoma at that time. The child was absolutely normal clini-cally and was discharged. He was symptom free during the next six months after the discharge and did not attend the clinic for follow up. During the second episode of left sided hemiparesis, complete hemogram was found to be normal with hemoglobin –10.6 mg/dL and platelet –3.6 lacs/cmm. BT, PT, APTT, were within normal limits. Blood urea, creatinine, electrolytes, blood sugar, X-ray chest, USG whole abdomen, urine for routine examination were normal. Urinary VMA was normal (4 mg/dL). CT scan brain showed ill defined mass in the right temporo-parietal region. MRA of brain showed no arterio-venous malformation and aneurysm, right middle cerebral artery was pushed upwards (Fig. 1). T2 weighted MRI of brain showed a variegated hyperdense mass with a horizontal level of contrast enhancement in the dependent part occupying the right temporo-parietal region along with mass effect suggestive of glioma, probably glioblastoma multiforme (Fig. 2). Histology showed fibrillar astrocyte with some primitive form along with fair number of tumor giant cells with areas of hemorrhage and necrosis. There was hyperplasia of vascular endothelial cells. The histological diagnosis was glioblastoma multiforme.
The child was prepared for ‘debulking operation’, but only biopsy could be taken due to low general condition of the child. The child was managed conservatively with anti-edema and anti-convulsant drugs, but succumbed to death within a few days. Discussion Intracranial tumors like pituitary adenoma, glioblastoma multiforme, medulloblastoma and metastatic tumors such as malignant melanoma, choriocarcinoma, renal cell carci-noma, bronchogenic carcinoma and germ cell tumors are a well recognized but uncommon cause of intracranial hemorrhage(1,2). In brain tumors other than pituitary adenoma, the incidence of hemorrhage is significantly higher in the patients under 14 years age(2), as in our case. This hemorrhage is commonly intra-tumoral than intracerebral. Hemorrhage occurring in glioblastoma multiforme are frequently deep into the hemisphere, basal ganglia or corpus callosum. Initial improvement in our case was due to resolution of the intratumoral hematoma. The tumor was present but due to its small size and temporal location no clinical manifestations were found within the next six months and it was not detected radiologically. Being the non-dominant hemisphere speech and audio psychic areas were also not affected. After six months, again when there was a second intra-tumoral bleeding, the tumor which had increased in size, along with the hemorrhage, produced a large space occupying lesion. It thus caused its mass effect and gradually resulted in tentorial herniation (due to increased intracranial tension) The characteristic variegated appearance of the mass with areas of necrosis and hemorrhage on MRI of brain suggested that it was possibly glioblastoma multiforme which was subsequently proved histologically. The incidence of glioblastoma multiforme per 1,00,000 population is 0.2 in the under 14 year age group and with increasing age its incidence increases(3). Most of the glioblastoma multiforme arise from the white matter and quickly infiltrate the brain extensively, sometimes attaining enormous size before attracting medical attention(3,4). The initial symptoms of the tumors when it is of any size may be a seizure or personality disorder. The commonest neurologic feature inpatient with glioblastoma mutiforme at presentation is hemiparesis(5). Approxi-mately 6% of patients with glioblastoma multiforme present with the acute onset of symptoms secondary to intacranial hemorr-hage and have a poor prognosis(5). Except for palliation, little can be done to alter the course of glioblastoma multiforme. Anti-edema therapy with anticonvulsants and partial resection of the tumor (‘debulking’) prolongs survival marginally(4). Less than one-fifth of all patients survive for one year after the onset of symptoms and only about 10% live beyond 2 years(3). Cerebral edema and raised intracranial tension are usually the immediate cause of death(3) as in our case. Intracranial hemorrhage should be suspected of being due to brain tumor in children in absence of common causes like cerebral aneurysm, vascular malformation or hypertensive cerebrovascular disease. Contributors: SDK contributed to case management, writing of manuscript and approved the final draft. AD was responsible for the clinical work up of the case. Funding: None. Competing interest: None stated.
| ||||
|
References | ||||
|
![]()