|
|
Brief Reports Indian Pediatrics 2005; 42:1013-1018 |
||||||||||||||||||||||||||||||
|
Myocardial Ischemia Induced by Nebulized Fenoterol for Severe Childhood Asthma |
||||||||||||||||||||||||||||||
|
L.Z. Zanoni, D.B. Palhares and L.C.T. Consolo From the Department of Pediatrics, Hospital Universitario, Universidade Federal de Mato Grosso do Sul, Campo Grande, Brazil. Correspondence to: Dr. Lourdes Zelia Zanoni, Rua Alexandre 378, Giocondo Orsi, CEP -79022-080, Campo Grande, Mato Grosso do Sul, Brazil. E-mail: [email protected] Manuscript received: February 23, 2004, Initial
review completed: May 20, 2004;
Severe acute asthma is characterized by increased airway obstruction, increased respiratory effort, and a mismatching of ventilation and perfusion, conditions that can lead to hypoxia, fatigue of the respiratory muscles, carbon dioxide retention, and respiratory acidosis(1). The use of aerosols has been recognized as the main procedure for treating severe, asthma exacerbations. Once inhaled, aerosols are deposited directly on their sites of action in the airway(2), with less systemic side effects(3). Several studies suggest that continuous nebulization of b2 adrenergic agonist may be more effective than intermittent nebulization in the treatment of severe asthma(4-6). These beneficial effects, however, have also been accompanied by systemic and metabolic reactions, and by electrocardiographic changes such as a flattening of T waves, depression of the ST segment, or prolongation of the QT interval, all dependent on the doses administered(7,8). Katz, et al.(9) demonstrated an increase in the MB fraction of creatine kinase, although without electro-cardiographic signs of myocardial ischemia, upon inhalation of albuterol at 0.5 mg/kg/dose. Several studies described complications associated with the use of nebulized albuterol(6, 9). The purpose of the present study was to examine for the occurrence of myocardial damage, alterations of the heart rate, cardiac enzymes creatine kinase, creatine kinase MB fraction and troponin induced by continuous inhalation of fenoterol in children with severe acute asthma. Subjects and Methods This study included 30 patients (17 boys) with severe acute asthma presenting to the Pediatric Emergency Division of University Hospital – the teaching hospital of Universidade Federal de Mato Grosso do Sul (UFMS), in Campo Grande, MS, Brazil, from August 1998 to December 2000. The patients were receiving no other therapies before the beginning of this study. The Medical Ethics Committee of UFMS approved the research protocol. Participation was allowed following informed parental consent was obtained. All information was supplied regarding the therapeutic approach to be employed, as well as on the possibility of side effects. Children with cardiac, muscular, renal or neoplasic illnesses did not take part in the study. Guidelines for the diagnosis and management of asthma(1) were used for the clinical diagnosis and estimation of the severity of acute exacerbation of asthma. All patients were given inhalation by employing a facemask, under a 6 L/min compressed air flow(10). A 0.5% solution of fenoterol hydrobromide was administered at a 0.5 mg/kg/dose (15 mg maximum) diluted in 30 mL of 0.9% saline solution, for one hour. Heart rate was measured by direct readout from a cardiac monitor at three different times: at admission, at the end of inhalation (60 minutes) and one hour after inhalation was completed. A 12-lead EKG was recorded for all patients, before inhalation and immediately after its completion. Myocardial ischemia was defined when any of the following criteria were present: occurrence of Q waves; ST-segment elevation; downsloping ST-segment depression of at least 1 mm at the J-point origin; horizontal ST-segment depression of at least 1 mm, 0.08 seconds or longer after the J-point origin; or slow upsloping ST-segment with a depression of at least 1.5 mm, 0.08 seconds or longer after the J-point origin. The EKG were analyzed by a cardiologist who was blinded to the patient conditions and therapy. Blood samples were obtained for quantifying the cardiac enzymes creatine kinase (CK), creatine kinase MB fraction (CK-MB), and troponin. CK and CK-MB levels were measured spectrophotometrically at admission and 12 h after treatment, by using the kinetic method (Granutest 2.5 plus-CK-MB DS kit, Merck KgaA). Total CK <225 IU/L and CK-MB <25 IU/L were considered normal for children. Troponin T was measured in 15 cases, 12 h after beginning of treatment using an inununologic test (Trop T sensitive Test, Boehringer Mannheim, UK). A positive result meant that troponin T concentration in the sample exceeded 0.1 ng/mL, indicative of myocardial damage(11). Statistical analyses were done on the data and expressed as mean, standard deviation, and percentages. Wilcoxon signed rank test(12) was applied for comparing differences before and after treatment. Stataquest 4.0 for Windows 95 software (serial number W-902103040, Stata Corporation, TX, USA) was employed for all statistical tests. Results At the end of fenoterol inhalation 8 patients failed to respond to therapy and were assessed as severe asthma. Of 22 patients that improved, 18 were assessed as moderate and 4 with mild asthma. Ages ranged from 2 to 11 years (mean 5.26 ± 2.6 years). Heart rates varied as shown in Table I. TABLE I
SD: Standard deviation; * compared to before treatment.
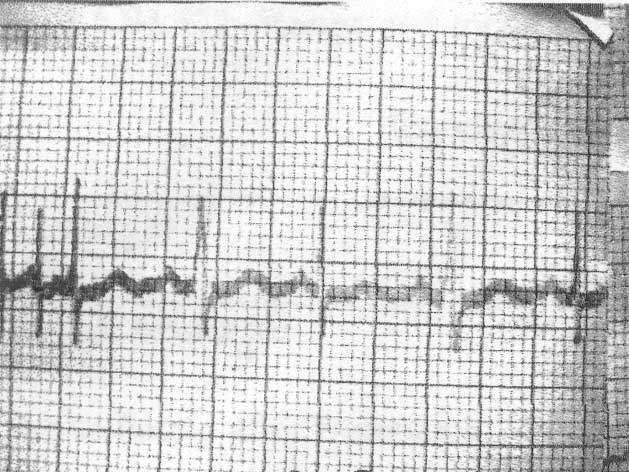
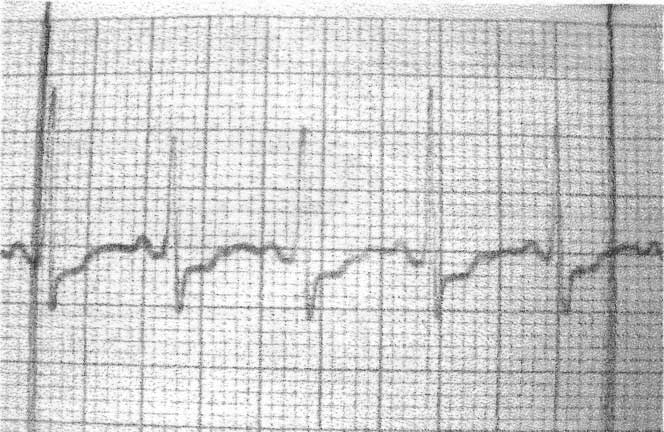
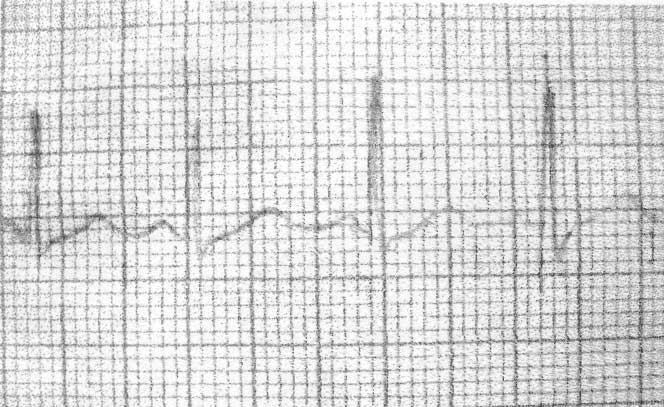
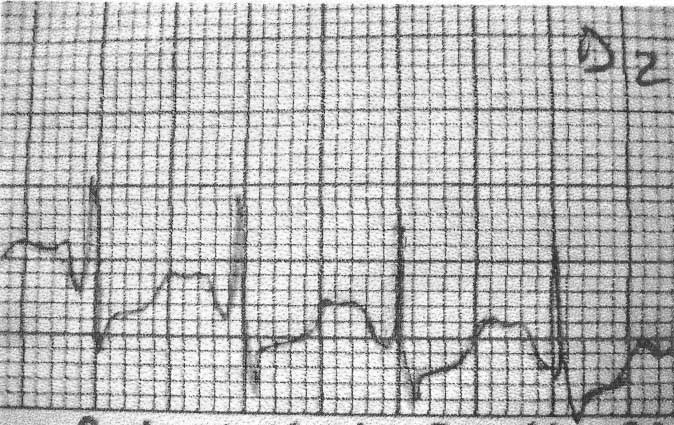
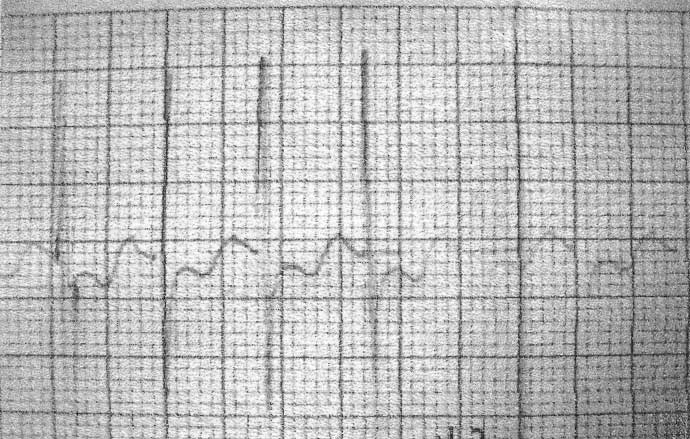
In six patients (20%), the changes observed on the EKG were compatible with myocardial ischemia. ST segment depression with straightening beyond 0.08 seconds was found in three patients (10%) (Fig. 1); slow upsloping ST-segment depression beyond 0.08 seconds in one patient (3.3%) (Fig. 2) and downsloping ST-segment depression beyond 0.08 seconds in two patients (6.6%) (Fig. 3). At the end of fenoterol inhalation, 2 had severe asthma and 4 had moderate asthma.
Prior to continuous inhalation of fenoterol, the mean CK concentration was 90.36 ± 43.9 IU/L (20.6-193.9 IU/L), which reduced to 80.6 ± 59.2 IU/L (16.5-342.5 IU/L) 12 h after treatment (P = 0.005). Only one patient (3.3%) showed CK concentration above normal levels. Prior to inhalation, the mean CK-MB concentration was 12.8 ± 82 IU/L (4.1-45.9 IU/L), which increased to 13.4 ± 11.3 IU/L (2-52 IU/L) (P = 0.5). Following inhalation, two patients had CK-MB concentrations above normal levels (41.8 and 31.2 IU/L, respectively). All 15 patients who were tested for the presence of troponin T in serum showed negative results. Discussion Although asthma is a frequent disease in childhood, acute episodes can lead to fatal outcomes many of which are potentially avoidable if the severity of the acute attack is recognized early, either by the patient, family or physician. Since the reduction in airway diameter allows only nearly 10% of inhaled drug doses to reach the lungs(13), high doses of β2 adrenergics have generally been used to ensure bronchodilation(9,14 ). EKG signals indicative of myocardial ischemia during the use of intravenous isoproterenol in children with severe acute asthma were reported by Maguire, et al.(15). In another study, continuous inhalation of albuterol resulted in increased CK-MB concentrations in 2 children without any EKG evidence of myocardial ischemia(9). Papo, et al.(6) did not report changes in either EKG or cardiac enzymes following albuterol inhalation in children. Of 17 children studied by Craig, et al.(16), an increase in CK-MB levels was found in only one patient. In the present study, CK concentrations reduced significantly from their initial values, excluding significant myocardial ischemia or necrosis. It is speculated that the decrease in total CK levels might be due to a decrease in respiratory effort following fenoterol inhalation(17,18 ). Regarding CK-MB, no statistically significant differences were found between measurements taken before treatment and after 12 h. When cases were analyzed individually, it was found that CK-MB levels had increased in the second measurement for three patients, only one of whom was tested for troponin, with negative result. It is worth mentioning that these patients did not manifest precordial pain or any EKG signs of myocardial ischemia or necrosis. CK-MB present in skeletal muscles accounts for 1-3% of total CK, whereas that present in the myocardium accounts for around 20% of the total(18). Further studies are needed for clarifying the cause of increased serum levels of CK-MB in children with acute asthma episodes, as well as the actual clinical meaning of this increase. In the present study, all patients tested for cardiac troponin showed negative results, which confirms the absence of myocardial necrosis. EKG showed an abnormal depression of the ST segment compatible with myocardial damage in 6 subjects, although cardiac enzymes were not elevated. Only two patients were tested for troponin T, with negative results. Although the children included in this study were not part of the population under risk for coronary artery disease, the EKG sign should not be ignored, since they may be indicative of subendocardial ischemic damage. In severe acute asthma, the combination of hypoxemia, use of b2 adrenergics and tachycardia might lead to increased myocardial workload, which favors myocardial ischemia and EKG signs of ischemic damage. It is likely that the lack of correlation of EKG findings with cardiac enzymes can be ascribed to the absence of myocardial necrosis; a feature that enables a diagnosis similar to that of angina pectoris(19). In children with an acute exacerbation of asthma, the coexistence of hypercapnia, hypoxemia, increased heart rate and EKG changes may be associated with a potential risk for severe cardiac arrhythmias when high doses of b2 adrenergics are inhaled. Further studies are needed to verify the duration of these EKG changes and the risk of continuous fenoterol inhalation. Continuous inhalation of fenoterol in the doses employed in this study must be performed in a hospital setting with clinical, hemodynamic and EKG monitoring, in order to minimize its potential for cardiotoxicity. Contributors: LZZ, DBP and LCTC were involved in conception and design of the study. LZZ collected interpreted and analyzed the data and will act as guarantor of the study. Funding: Federal University of Mato Grosso d sul. Competing interests: None.
| ||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||
![]()