|
|
Review Article Indian Pediatrics 2004;41:1008-1017 |
||||||||||||||||||||||||||||||||||||||
D. Millar*
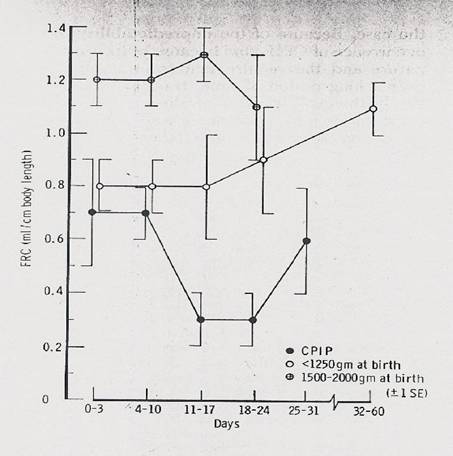
Abstract Mechanical ventilation of the newborn infant has increased neonatal survival. However, this increased survival has come at the expense of increased morbidity, in the form of bronchopulmonary dysplasia, and at the cost of an expensive technology. Continuous positive airway pressure (CPAP) is accepted as conferring clinical benefit in supporting the recently extubated preterm infant and in the management of apnea of prematurity. Attention is now being drawn to physiologic and clinical evidence to support CPAP use, with or without early surfactant, as a primary treatment of hyaline membrane disease. The purpose of this review is to explore these proposed benefits of non invasive ventilation and place them in the context of current clinical evidence. Key words: Artificial respiration; Broncho-pulmonary dysplasia; Continuous positive airway pressure. Ventilation of the newborn infants, although potentially life saving, is not free of associated morbidity. In preterm infants, this morbidity is largely due to bronchopulmonary dysplasia (BPD). Ventilation is one of the more expensive therapies in neonatal intensive care. A term infant with respiratory failure, requiring mechanical ventilation, costs in North America (in 2002 US$) $4560 for the first day, and $1920 for subsequent days, excluding physician costs(1). The most expensive item, other than equipment, is nursing and respiratory practitioner labor, the cost of which admittedly does vary worldwide. An ideal ventilation strategy would reduce the incidence of BPD, be easy to use, require minimal training and be inexpensive. This ideal strategy would be of benefit to both the developing and developed world. Could non-invasive ventilation be a part of this ideal solution? Bronchopulmonary dysplasia The developing lung of the preterm infant is delicate and easily injured by the therapies necessary to sustain ex-utero life. Broncho-pulmonary dysplasia (BPD), is characterized by early interstitial and alveolar edema which progresses to persistent inflammation and fibrosis. Infants with BPD have a higher mortality and morbidity; they receive more ventilation, drugs, oxygen and intensive care and have higher hospital readmission rates in the first year of life than infants, of similar gestational age, who do not develop BPD(2). As the survival rate of preterm infants improves, the incidence of BPD rises: current trials estimate an incidence of 45% in ELBW infants(3). Both antenatal steroids and surfactant have altered the clinical presentation and hence the definition of BPD. These previous definitions, stressed an early period of ventilatory support in hyaline membrane disease (HMD), followed by prolonged exposure to ventilation and oxygen(4). Increasingly a different picture – "new BPD", is noted in ELBW(5) in the first days to weeks of life, infants may require no or modest respiratory support, which only becomes necessary later. This "new BPD", of ELBW infants, reflects injury to an immature lung, during the saccular stage of development. Interestingly, a generation ago Krauss, et al. described the fall in functional residual capacity (FRC) of ELBW infants who developed respiratory symptoms over the first 2 weeks of life, compared to similar birth weight infants with no respiratory signs and a cohort of higher birth weight infants(6). Krauss’s infants with chronic pulmonary insufficiency of prematurity (CPIP) are very similar to infants in the current ‘epidemic’ of the new BPD (Fig. 1). A common theme appears to be atelectasis, which then requires "re-expansion", leading to atelectatic areas and areas of over-distension.
Conventional mechanical ventilation via an endotracheal tube, enabling adequate gas exchange, has undoubtedly led to improvement in neonatal survival in the last thirty years. However, the prolonged use of an endotracheal tube and mechanical ventilation may cause upper airway damage, alter normal mucociliary flow, lead to infection and predispose the infant to BPD(4,7). While multiple factors contribute to BPD, intubation and mechanical ventilation of preterm infants remains the single most important predictor of subsequent BPD(8,9). The ventilatory risk factors for lung injury are volutrauma, barotrauma and atelectasis or end-expiratory alveolar collapse. These factors are not mutually exclusive as readily appreciated by the relationship between a driving pressure and the volume it recruits would indicate. These mechanical stresses are transduced into a final common biological signal via toxic reactive oxygen species, and associated inflammation. This is recognised in the nomenclature of ventilator-induced lung injury (VILI). Since the structural abnormalities of injured lungs cannot be easily reversed, preventive measures aimed at minimising the incidence and severity of BPD are very attractive. For this review, we focus on the key mechanical aspects to avoid volubarotrauma and atelectasis. "Open the lung and keep the lung open" In 1992 Lachmann coined this phrase to highlight a ventilation strategy for adults with adult respiratory distress syndrome (ARDS)(10). The main thrust of this ventilatory strategy is aimed at preventing partial or complete end-expiratory lung collapse (atelectasis). While the concepts of high volume and high pressure injury were commonly understood, Lachmann’s phrase encapsulated the problems of "low volume injury" or atelectasis, raising important issues about recruitment. Although primarily applied to adult lung strategies, the term has special resonance to neonates, because the preterm infant’s thorax is unique, exhibiting problems in maintaining end-expiratory lung volume or FRC. The musculoskeletal thorax is meant to oppose lung collapse, but in preterms the chest wall is highly compliant, compared to the adult or older child’s ‘exoskeleton’. In addition, when surfactant deficiency is present, with a diminution of surface tension, this leads to further collapse of alveolar segments(11). Both the increased thoracic compliance and surfactant deficiency, lead to a loss of FRC, forcing the infant to attempt gaseous exchange in a smaller compartment of ventilated lung. This expansion and contraction of lungs below a "normal FRC" will result in cyclical opening and closing of lung units, with ensuing injury(12). This low-volume injury or atelectotrauma leads to inflammatory changes preceding BPD. Compounding these problems is the ready fatiguability of the respiratory muscles of preterms. Their diaphragms have a lower number of high-oxidative fibers; rendering them at risk of fatigue. Muller, et al. using EMG via surface electrodes demonstrated that normal preterm and term infants’ diaphragms operate very close to the threshold of diaphragmatic fatigue(13). Respiratory support aims to increase and maintain FRC, prevent atelectasis (augmenting surfactant production), support the easily fatigueable ventilatory muscles, and provide respiratory stimulation (against apnea): and in doing so, provide gaseous exchange. Could non-invasive ventilation achieve these desirable qualities? Continuous Positive Airway Pressure (CPAP) Concerns about the ‘epidemic’ of BPD have driven a resurgence in the use of CPAP. CPAP delivers a continuous distending pressure via the infant’s pharynx to the upper and lower airways. The first reported use of CPAP in the neonatal population, for the treatment of HMD, was by Gregory et al. in 1971(14). In respiratory failure, CPAP is used in spontaneously breathing infants to prevent alveolar atelectasis, enhance and maintain FRC and reduce the work of breathing(15). It has a number of potential physiologic benefits, both in respiratory failure and apnea of prematurity, which is the other main indication for its use(16). Table I tabulates both animal and human data. Table I Physiologic Benefits of Continuous Positive Airway Pressure
Since its introduction, more than thirty years ago, CPAP devices have proliferated and currently there are a large number of potential delivery systems and flow drivers. Fundamentally, however, the delivery of continuous positive airway pressure requires three components: 1. Flow generation; 2. An airway interface; 3. A positive pressure system. Flow Generation Two major varieties exist; constant flow and variable flow (demand). The flow generator usually also warms and humidifies the inhaled gases. Constant flow is usually provided by an infant ventilator; which because it can be used in two ways, may limit expenditure on hardware. Most often, the amount of flow is set by the clinical team. Alternatively, variable flow devices use a dedicated flow generator. Here the "expiratory" limb of the circuit is open to the atmosphere and the infant can draw extra gas from this limb to support inspiratory efforts. This device has gained widespread acceptance in Europe and North America(17). Despite the theoretical advantages of the variable flow device, there are no consistent data showing clinical long-term meaningful benefit over constant flow devices(18). Airway Interface A bewildering array of interfaces between the circuits and the infant’s airway are in use: single prongs, binasal prongs (short & long), nasopharyngeal prongs, endotracheal tubes, head boxes, pressurised plastic bag, nasal cannulae and face masks. The most commonly used route today - nasal CPAP, was introduced in the early 1970s. Nasal prongs are very easy to apply and comparatively non-invasive to the airways. The infant can still be nursed and handled with uninterrupted CPAP. A Cochrane Systematic Review suggests that short binasal prongs are more effective, in preterm infants, at preventing re-intubation compared to single nasal prongs(19). Nasal prongs can, however, cause nasal excoriation and scarring(20). The use of nasal cannulae is effective in the treatment of apnea of prematurity(21), however there still may be associated nasal mucosal trauma and bleeding. Positive Pressure System At its simplest, an oscillating, expiratory pressure is provided by a fluid column (bubble CPAP)(22); more frequently, by resistance applied at the expiratory valve of the ventilator; by a Benveniste device - pressure generation at nasal level(23); or by generating CPAP in the immediate vicinity of the nasal airway by converting kinetic energy from a jet of fresh gas (Infant Flow System)(24). Bubble CPAP delivers mechanical oscillatory vibrations which are transmitted into the chest secondary to the non-uniform flow of gas bubbles across a downstream underwater seal. Its proponents point to generated waveforms, in the airway similar to those produced by high-frequency ventilation(22). In preterm lambs, bubble CPAP results in lower indicators of acute lung injury (neutrophils and hydrogen peroxide) than mechanical ventilation in the first two hours of life(25). Using bubble CPAP, in an historical cohort study, the same group demonstrated reduced days on mechanical ventilation and postnatal steroid use in the NICU for ELBW infants(26). Bubble CPAP has the advantage of being simple and inexpensive. The Infant Flow System uses unique fluid mechanics to adjust the gas flow throughout the respiratory cycle; this "fluidic flip" action has been reported to reduce work of breathing, by reducing expiratory resistance and maintaining a stable airway pressure throughout respiration(24). Studies are required to identify the most effective pressure source for supplying continuous distending pressure. Optimal Pressure There are no compelling data about the optimal pressures for CPAP in infants. Traditionally, pressures of 4 - 6 cm H2O have been used. Some investigators, however, claim that higher pressures should be used and some studies have used pressures as high as 10 cm H2O(27). Clinically, we suggest tailoring pressure to the infants needs - titrating pressures against parameters such as: increasing oxygen requirements; increase in apneic episodes; increase in work of breathing; appearance of low volume lung fields on chest radiograph. All these should prompt a judicious increase in the distending pressure by 1 cm H2O increments to a maximum of 10 cm H2O. There are few clinical studies on this question, although older physiologic studies, with monitoring of esophageal pressures, would support this approach(28). Indications for CPAP (Table II) Table II Indications for CPAP
CPAP is now used for a variety of neonatal conditions. It is effective in supporting the recently extubated infant(29) and for treating apnea of prematurity(16). Increasingly, it is seen as an alternative to intubation and ventilation in the treatment of HMD. Coupling CPAP with short duration intubation and early delivery of a single dose of surfactant, for moderate to severe HMD, improves oxygenation and reduces the need for mechanical ventilation(30). This approach has become known as the INSURE technique (Intubation; Surfactant; rapid Extubation). In historical case series, the team at Columbia University has consistently demonstrated a decreased prevalence of BPD,(8;9) compared to other NICU centers. This was credited to a management strategy emphasizing early and routine use of CPAP, for the treatment of HMD, and more limited use of intubation, surfactant and mechanical ventilation, but was never subject to a randomized controlled trial. Conditions where CPAP may not be useful include upper airway abnormalities (e.g. Pierre-Robin Sequence), severe cardio-vascular instability and intractable apneic episodes. Practical Considerations The use of CPAP requires meticulous attention to the infant’s airway. Both the correct prong size and proper positioning of the infant’s neck are needed to avoid excessive flexion or extension. Optimal humidification of the inhaled gas should be ensured and the airway requires frequent suction to clear accumulated secretions, although how often this is needed has not been studied. An oral gastric tube will help relieve gaseous distension of the bowel. Robertson et al. demonstrated, in a cohort of infants requiring CPAP, that 20% had nasal complications - columella nasi necrosis, flaring of the nostrils and snubbing of the nose(20). Observation and care of the nasal area is important in the nursing care of infants requiring nasal CPAP. Clinicians should be aware that CPAP has been associated with more serious complications including pneumothoraces and air embolism(31,32). Therefore all infants needing respiratory support, be it invasive or non-invasive continue to require careful monitoring for clinical deterioration. No compromises for CPAP should be made in this regard, and CPAP usage requires constant observation of breathing patterns and standardized and rigorous training of physicians, respiratory practitioners and nursing staff. Developing World and CPAP Many infants, with higher mortality and morbidity, are denied access to neonatal intensive care in the developing world because "scarce" financial resources are directed towards more viable infants. In a prospective study, from South Africa, Pieper et al. conducted a quasi-randomized control trial of CPAP for infants, birth weight 775 - 1160 g, denied access to NICU compared to the standard therapy of headbox oxygen(33). Although the CPAP was initially placed by respiratory therapists, the ongoing care was continued by nursing staff with no intensive care or CPAP experience. The infants who received CPAP in these circumstances had a significantly improved short term survival (at 24 hours), with trends towards improved long-term survival. None of the infants in the study received surfactant therapy. Could the routine early use of CPAP in areas of diminished neonatal resources provide an alternative to conventional mechanical ventilation? Only a properly conducted randomized control trial can provide the answers. Practical Aspects of Setting up a CPAP System The simplest and least expensive nasal CPAP system, to set up, is the bubble CPAP system (Fig. 2). One requires the equipment shown in Table 3.
Table III–Equipment for CPAP
Fill the container with sterile water to 10 cm H2O and place the container below the level of the infant. The column should be fitted into the container through the lid and placed under the fluid level to desired pressure i.e., initially 6-7 cm H2O; the expiratory circuit from the infant is connected to the column. The expiratory circuit will need a port and pressure tubing leading to a calibrated manometer. Snug fitting short, anatomical nasal prongs are secured with a bonnet and the inspiratory circuit is connected to the oxygen supply, flow meter, blender and analyzer via a humidified heater. A starting flow of 6L per min should be used, increasing to produce a steady stream of bubbles in the water container. The column can then be lowered or raised to the desired pressure to ensure steady bubbling. Nasal Intermittent Positive Pressure Ventilation (nIPPV) A newer strategy has used nasal intermittent positive pressure ventilation, via nasal prongs, with and without synchronization as an alternative non-invasive strategy for respiratory support. Synchronization in this context has usually been provided by an abdominal sensor. Nasal IPPV may improve patency of the upper airway by creating intermittently elevated pharyngeal pressures. This intermittent inflation of the pharynx may activate respiratory drive, by Head’s paradoxical reflex, where lung inflation provokes an augmented inspiratory reflex. Physiologically, synchronized nasal intermittent positive pressure ventilation (sNIPPV) may offer advantages over nCPAP, by improving tidal and minute volumes and by activating respiratory drive which is poorly controlled in extremely low birth weight infants. Three randomized control trials are published, demonstrating that sNIPPV provides superior respiratory support, compared to CPAP, for recently extubated preterm infants(34) with a number needed to treat (NNT) of 3 infants treated to prevent one extubation failure. A trend towards lower rates of BPD in infants randomized to sNIPPV was noted in the two trials reporting this outcome, but the trials were not sufficiently powered. There are no studies describing the use of sNIPPV in the first line management of hyaline membrane disease. We cannot tell if the advantages of sNIPPV in the short term over CPAP following extubation lead to real and meaningful clinical outcomes in the longer term. Continuous Negative Extrathoracic Pressure (CNEP) During the polio epidemics of 1930 to 1960 negative pressure ventilators in the form of the "iron lung" saved many lives. However, by the 1950s the greater efficiency of positive pressure ventilation through a tracheostomy or endotracheal tube had superseded the negative pressure devices. Despite one modern randomized controlled trial on CNEP(36) in neonatal respiratory failure, showing a small benefit the devices have failed to gain widespread acceptance and have been superseded by more effective nasal CPAP. Summary Concerns about the damaging effects, and expense, of conventional mechanical ventilation have led neonatologists to seek new methods of respiratory support for the preterm infant such as non-invasive respiratory support. Non-invasive pressure support is useful because it can limit lung injury; namely, volu-barotrauma and atelectotrauma. Both CPAP and nasal IPPV have desirable physiologic properties: - maintaining FRC, recruitment, decrease upper airway collapse and promoting the release and conservation of surfactant. CPAP is effective in preventing extubation failure and also in the management of apnea of prematurity. Whether sNIPPV has further clinical benefit, over and beyond CPAP alone will depend on whether superior maintenance of lung volume and decreased work of breathing, translate into meaningful clinical benefits such as reduced BPD and/or time on ventilator. The decreased capital outlay of CPAP systems coupled with a standardized training for physicians and nursing staff, may be of benefit in the developing world with finite finances for supporting preterm infants. Further references to accompany this article are available from the corresponding author. Contributors: Both authors contributed to the concept and design of the article and the drafting and revision thereof. Funding: None. Competing interests: None.
| ||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||
![]()