|
|
Case Reports Indian Pediatrics 2001; 38: 1185-1189 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Tricuspid Regurgitation in a Pair of Twins at Birth Secondary to Antenatal Indomethacin |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
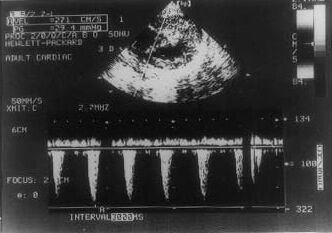
Indomethacin, a prostaglandin synthetase inhibitor, gained popularity in the early 1970s as an effective tocolytic agent for preterm labor(1). This popularity, however, decreased after several case reports indicating an increase in the incidence of fetal and neonatal complications associated with Indomethacin use(2-5). Such complications included hyper-bilirubinemia, necrotizing enterocolitis, intra-ventricular hemorrhage and oligo-hydram-nios. Of particular concern were reports of fetal ductal arteriosus constriction with resultant pulmonary hypertension. In the mid 1980s several authors reported supportive clinical trials for the safety and efficacy of indomethacin when used for short-term toco-lysis at a gestational age of <34 weeks(6,7). It was shown that ductal constric-tion is reversible after prompt identification and discontinuation of indomethacin. Hence, it was thought indomethacin can be safely used in pregnant mothers before the gestational age of 32 weeks with serial weekly fetal echocardiography(8). We report a case of twin gestation that received indomethacin for only 7 days and had ductal constriction in both fetuses that resulted in transient tricuspid regurgitation in bot h the neonates. Case Report A mother was admitted at 27 weeks of gestation with twin gestation, polyhydram-nios and premature labor. She received isoxsuprine to suppress premature onset of labor. Obstetric ultrasound revealed severe polyhydramnios. She underwent therapeutic amniocentesis on day 2 and day 5 of admission, but polyhydramnios persisted and it was decided to use indomethacin for the treatment of polyhydramnios. Fetal echo-cardiography was done before starting indomethacin, which was normal. She was started on oral indomethacin 25 mg four times daily for 7 days. The fetal echocardiography, which was done on 10th day of starting indomethacin showed evidence of dilated right atrium, dilated right ventricle and tricuspid regurgitation in one fetus. Ductal signal could not be obtained in the fetus. Echocardiography done two weeks later showed similar finding. Echocardiography done 1 week later (10 days before delivery) showed evidence of severe tricuspid regurgitation and peak systolic velocity in ductal signal was 115 cm/sec (Table I). She developed oligohydramnios at 33 weeks of gestation, which became severe at 35 weeks. Pregnancy was terminated at 35 weeks of gestation in view of severe oligohydramnios. Induction of labor was done with oxytocin and both neonates were delivered vaginally. First baby’s weight was 1900 grams and had apgar of 7 at 1 minute and 8 at 5 minutes. This baby developed respiratory distress at 10 minutes of life. Test for surfactant maturity showed immature shake test. Surfactant was given at 20 minutes of life and baby was ventilated with nasopharyngeal CPAP for 18 hours. Examination of baby revealed tachy-cardia, tachypnea, facial puffiness, and edema of the limbs, systolic murmer, and hepatomegaly. Chest X-ray revealed cardio-megaly. ECG showed right ventricular and right atrial hypertrophy. Neonatal echo-cardiography done at 24 hours of life demonstrated severe tricuspid regurgitation (Fig. 1). Her congestive cardiac failure became passive on day 3 of life. Repeat echocardiography on day 4 showed moderate tricuspid regurgitation. Baby was discharged on day 11 of life. In follow up, on day 33 of life tricuspid regurgitation could not be detected on echocardiography (Table I). The second twin was 1200 grams at birth, had Apgar of 7 at 1 minute and 9 at 5 minutes of life. This baby also had respiratory distress that appeared at 10 minutes of life and received surfactant at 30 minutes of life. Respiratory distress became passive at 8 hours of life. There was no evidence of congestive cardiac failure in this baby; however, neonatal echocardiography done at 24 hours of life showed evidence of mild tricuspid regurgitation. Repeat echocardio-graphy on day 4 was normal (Table I).
RAP – Right atrial pressure; TR – Tricuspid regurgitation; RVSP – Right ventricular systolic pressure. Discussion Prostaglandin synthetase inhibitors given to the pregnant ewe(9,10) have been shown to constrict the fetal ductal arteriosus. This results in fetal pulmonary arterial hyper-tension, which has been shown to cause the development of excessive pulmonary arterial smooth muslce. Acute degenerative changes in the tricuspid valve papillary muscle, the right ventricular free wall and inter-ventricular septum have been shown to occur in fetuses in animal studies secondary to the ductal constriction induced by indomethacin when given to pregnant animals(11). It has also been suggested that if this ductal constriction is severe, it can cause fetal death. If less severe, this mechanism may be the cause of tricuspid insufficiency due to papillary muscle infarction in the newborn period. Archill et al.(12) reported a newborn who had tricuspid insufficiency, severe heart failure, and acidosis at birth, which dis-appeared on next day. Hemodynamic studies at 4 hours of birth demonstrated a large cone shaped ductus arteriosus arising from pulmonary artery but ending blindly at its aortic end. These findings were considered consistent with isolated closure of ductus before birth. The mother had received high doses of aspirin in antenatal period.
Fig. 1. Echocardiogram showing tricuspid regurgitation Vermillion et al.(13) showed that ductal constriction developed in 50% of fetuses exposed to indomethacin, ranging from 24 to 35 weeks of gestation. Ductal constriction was detected at a mean gestational age of 30.9 ± 2.3 weeks at an average of 5.1 ± 6.0 (range 1 to 27) days after initiation of therapy. Oligohydramnios occurred without ductal constriction in 2 cases, whereas both oligohydramnios and ductal constriction developed in 9 cases. There was no significant difference between singleton and multi fetal gestation with regard to incidence and timing of ductal constriction. Among twin gestation, both fetuses demonstrated ductal constriction in 5 of 7 cases. One of the two sets of triplets demonstrated ductal constriction; however, only one of the three fetuses was affected. After discontinuation of indomethacin therapy all follow up echocardiograms demonstrated the resolution of the ductal constriction. None of the newborn had any problem related to the ductal constriction. In the twin gestation constriction of ductus secondary to indomethacin occurred uni-formly between fetuses but with variation in severity. Moise et al.(14) reported 50% incidence of fetal ductal constriction in their study of 13 pregnant women treated with indomethacin. The gestational ages ranged from 26.5 to 31.0 weeks. Six of the seven fetuses, which developed ductal constriction, had evidence of ductal constriction within 24 hours of starting indomethacin. Repeat fetal echo-cardiography done 24 hours after stopping indometahcin showed resolution of ductal constriction in all the fetuses. None of these had any neonatal problem due to antenatal exposure to indomethacin. Dudley et al.(15) reported that none of the newborn had evidence of ductal constriction or persistent fetal circulation among the 167 fetuses exposed to antenatal indomethacin. Niebyl(16) also reported that none of the newborn exposed to antenatal indomethacin had ductal constriction. However, in both of these studies fetuses were not monitored for the evidence of ductal constriction antenataly. Both the babies had tricuspid regurgitation that resolved with time. Pulmonary hyper-tension is an important cause of tricuspid regurgitation. Pumonary vascular resistance which is very high in the fetus falls rapidly soon after birth and gradually reaches adult level by 2 to 4 weeks of life(17). The natural fall in the pulmonary vascular resistance is most probably the explanation of the resolution of tricuspid regurgitation with time in these two babies. This case reinforces the worry regarding fetal ductal constriction due to the use of indometahcin during pregnancy. If we have no choice other than using indomethacin during pregnancy, regular fetal echocardio-graphy should be done to detect the fetal ductal constriction at the earliest. It may be good practice to do the fetal echo-cardiography on day 2 of starting of indo-methacin, as at this time ductal constriction may be reversible. If fetus develops ductal constriction, regular follow-up with fetal echocardiography is necessary. Acknowledgement The authors are grateful to Prof. Anil Narang (Head, Neonatal Unit, Department of Pediatrics, PGIMER, Chandigarh) and Dr. Praveen Kumar (Associate Professor, Depart-ment of Pediatrics, PGIMER, Chandigarh) for their keen interest and help during the case management and the preparation of the manuscript. Contributors: RK collected the data and drafted the manuscript, he will act as the guarantor for the paper. YS and IG were involved in patient care and helped in drafting the manuscript. Funding: None.
References
|
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||