|
|
Case Reports Indian Pediatrics 2001; 38: 1177-1180 |
||||
|
Mediastinal Tamponade Following External Jugular Vein Cannulation |
||||
|
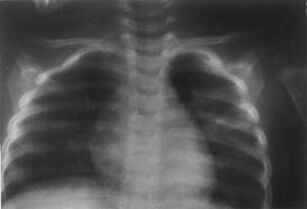
Complications of Central Venous Lines (CVLs) include pneumo and hemothorax, chylothorax, air embolism, pericardial tampo-nade, infections, hematoma, carotid and vertebral artery puncture, nerve injuries and Horner’s syndrome. Hydromediastinum and mediastinal tamponade are rare complica-tions. We report a case of mediastinal tamponade due to a cannula inserted in the right external jugular vein. Case Report A 1½-years-old child was admitted for dehydration, shock and severe metabolic acidosis. She was treated with ringer lactate, intravenous fluids and sodium bicarbonate. Because of persistent acidosis, she was put on a bicarbonate drip. With this treatment she recovered rapidly and acidosis was corrected. Because the first intravenous line was blocked, a cannula was put in the right exter-nal jugular vein at 12 noon and intravenous fluids were continued. At about 11 p.m. it was discovered that the patient had suddenly deteriorated. There was tachycardia, tachy-pnea, feeble pulses, low blood pressure and heart sounds were distant. There was no explanation for this sudden deterioration in the patient’s condition. The ABGs were normal, there was no acidosis and oxygen saturation was normal. So some complication of central venous line, such as pericardial effusion or hemorrhage was suspected. A chest X-ray was done which showed (Fig. 1) grossly widened superior mediastinal shadow, enlarged cardiac shadow, bilateral lamellar pleural effusions, and effusion in the right oblique fissure. Right lamellar effusion appeared contiguous with the widened superior mediastinal shadow. CVL tip was seen in the right second intercostal space. The patient’s clinical condition and the enlarged cardiac shadow was suggestive of pericardial or mediastinal tamponade. Echocardiogram had revealed a small pericardial effusion. Pericardial tap through subxiphisternal route produced 7 ml of clear fluid. This did not make any difference to the patient’s condi-tion. Mediastinal effusion and tamponade now seemed to be the main cause of patient’s condition. It was decided to drain as much fluid as possible from the pleural cavities. Through right pleural aspiration, more than 500 ml of clear fluid (the intravenous drip fluid), was removed. With this the patient’s condition improved dramatically; tachycardia and tachypnea settled, blood pressure became normal and heart sounds became normally audible.
Chest X-ray taken after pleural aspiration also showed dramatic improvement (Fig. 2). The widened superior mediastinal shadow had become normal and narrow, most of the pleural effusion and the effusion from the oblique fissure had cleared. The fluid in mediastinal space was probably in commu-nication with pleural space and got drained through pleural tapping, thus improving the patient’s condition.
Discussion Various complications, some fatal, can result from these procedures. Yarom(1) was the first to warn of the potential dangers of subclavian vein catheterization. Internal jugular vein catheterization has many complications. Some rare ones include vertebral(2) and transverse cervical artery pseudoaneurysm, diaphragmatic paralysis(3), carotid artery and lymphatic vessel puncture, chylothorax(4) and hydrothorax(5). Reports of complications after external jugular venous cannulation are few. Hydromediastinum due to insertion of CVP line via the right external jugular vein has been reported(6). In our case right external jugular vein cannulation resulted in extensive extravastion of fluid in the mediastinum, compressing the vena cavae, aorta, pulmonary artery and veins. This extravasated fluid pressure reduced the right ventricular filling in diastole, with a resultant decreased stroke volume and cardiac output. Fatal mediastinal tamponade can occur if fluid infused through a catheter enters the mediastinum(6). This problem has been reviewed recently(7). The hemodynamic effects of mediastinal tamponade are the same as of cardiac tamponade. Tamponade should always be considered when a patient suddenly deteriorates hemo-dynamically after the placement of a CVL. The fluid leaking from a CVL accumulates slowly. The effects of extravasation of fluid are seldom seen in the emergency room or in the intensive care unit immediately after the introduction of CVL. This is because of the slow accumulation of the fluid. The effusion may eventually become tremendous in size and it may be several hours before the effects become apparent. This is precisely what happened in our case, after eleven hours. The basic pathophysiology and hemodynamic effects of accumulation of fluid in mediastinal space and in the pleural space are elevation of intrathoracic and intracardiac pressures, limitation of ventricular filling, and reduction of cardiac output. The three important signs of acute cardiac compression are raised central venous pressure, severe hypotension and muffled heart sounds. Other features include dyspnea, orthopnea, hepatomegaly and paradoxical pulse consisting of greater than normal 10 mmHg inspiratory decline in systolic arterial pressure. All these features are due to the basic pathophysiological process of impedance to the ventricular filling and reduced cardiac output. Rarely one finds all these signs in one patient and it would be imprudent to wait for all these classical signs to develop. The clinical diagnosis of tampo-nade requires a high degree of suspicion and awareness that this lethal complication is rarely possible, whenever a CVL is inserted. Contributors:
GG was responsible for managing the case and drafting the manuscript; he
will act as the guarantor. ASD helped in drafting the manuscript.
References
|
| 1. Sheep RE, Guiney WB. Fatal cardiac tampo-nade: Occurrence with other complications after left internal jugular vein catheterization. JAMA 1982; 248: 1632. 2. Aoki H, Mizobe T, Nozuchi S, Hatanaka T, Tanaka Y. Vertebral artery pseudoaneursym: A rare complication of internal jugular vein catheterization. Anasthesia Analgesia 1997; 75: 296-298. 3. Sanchez Castilla M, Lopez Martinez J, Rodriguez Tato P, Asuero de Lis MS. Paralisis diafragmatica post cateterizacion de la vena yugular interna. Nutr Hosp 1995; 10: 377-378. 4. Hsu LH, Lien TC, Wang JH Chung Hua I. Chylothorax: A complication of internal jugular vein catheterization. Hsueh Tsa Chih 1997; 60: 57-61. 5. Olivares Lopez A, Borras Rubio E, Sanchez Ortega JL, Fernandez Contreras R, Riquelme MR, Lopez Rodriguez F. Hidrotorax Yatrogeno tras la cateterizacion de la vena yugular interna izquierda. Rev Esp Anestesiol Reanim 1991; 38: 189-191. 6. Lee TS, Chen BJ. Hydromediastinum following insertion of a central venous pressure line via the right external jugular vein. J Clin Anesth 1993; 5: 436-438. 7. Roddies M, Alexander D, Mediastinal tampo-nade. Anaenesthesics 2000; 55: 705-760. |