|
|
Viewpoint Indian Pediatrics 2001; 38: 1129-1143 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Child Health Development After Alma Ata Declaration |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Health development includes health care, essential non-specific measures like nutrition, protected water supply, sanitation, education and economic development. Primary Health Care (PHC) is essential health care based on practical, scientifically sound and socially acceptable methods. Community involve-ment, inter sectoral cooperation and approaches to peripheralise health services are the three pillars on which PHC is being built. Implementing PHC successfully will improve health development. Human progress and overall development lie in the progress of women and children and the realization of their rights. Problems of health development and under development are intimately linked. In the later half of last century important technological advances in medicine were made. Vaccination against major diseases and therapy for infectious diseases and the technical knowledge to prevent nutrition deprivation and diseases were available. As a result rapid decline in death rate has occurred. Inspite of impressive progress in health picture, the prevailing health and nutrition disparities were a cause for serious concern. Medical science realized that poverty related social conditions like poor sanitation and housing were major causes of ill health. Studies have shown that irrespective of medical intervention health status improved remarkably when basic requirements of health were available. The challenge was primarily a question of equal access for all. In 1978 for the first time all the Government of the world - Democracies or Dictatorships, Communists or Capitalists - accepted the principle of PHC officially and promised to bring them into being in all nations within the next 22 years. This Alma-Ata Declaration accepted that Health is a Fundamental Human Right. It also accepted that the gross inequalities in health status are unacceptable. Health for all heralded the vision of a new and better future for all the human family. To fulfil her commitment of Health for All, India evolved a National Health Policy in 1983. To transfer all objectives of Health for All, the policy laid down specific goals with quantifiable targets to be achieved. This commitment did lead to some renewed attempt at achieving these goals. India launched ambitious campaigns for eradica-tion of communicable diseases, infections and malnutrition. Various policies and acts introduced earlier and later tried to augment efforts. Few examples in this context include ICDS (1974) CSSM (1992), The Infant Milk Substitute Act (1992), Pulse Polio Immunization (1997), RCH and others. The impact of all these interventions to improve health, particularly maternal and child health has been large. In India decline in vaccine preventable diseases and severe malnutrition of this magnitude has never been achieved in our setting and certainly not in an equivalent period of time. Still there are disparities in health. So the achievements of the National Health Policy need critical analysis. Progress in Maternal and Child Health A. Mortality and Mobidity in and around Infancy (Table I) Mortality rates and nutrition status are good indicators to measure the level of health and nutrition care. This also helps in assessing the overall socioeconomic development. Still births and deaths within the first week of life are not investigated like infant and neonatal deaths. With declining infant mortality rate, perinatal mortality is assuming importance as a yardstick of obstetric and pediatric care before and around the time of birth. There is a wide variation in urban/rural death rates. The target is still not achieved since the rate is 45/1000 live births. Deaths occurring 28 days after birth (neonatal mortality), contributes to 50 to 55% of infant mortality rate (IMR). Perinatal and neonatal deaths are largely the consequences of inadequate and inappropriate care during pregnancy, during the crucial first few hours after delivery. The causes of perinatal and neonatal mortality are multi-factorial and include low birth weight, neonatal asphyxia, birth injury, congenital malformations and infections. In India, tetanus neonatorum still accounts for neonatal deaths in some states. The rural rates are almost double that of urban rates. The high concentration in the early neonatal period suggests the need to improve maternal health. There was a decline in infant mortality in the eighties but the decline has been static for the last five years. The decline is mainly due to medical care and indicates the need to address endogenous and socio economic causes. The urban rural differences are obvious. In 1999 the urban rate was 44 and the rural was 74. The low rates in urban areas are due to access to better medical care. Deaths among girls is higher, indicating neglect of girl children. A high IMR is observed in infants born to very young and old mothers, illiterate mothers, and those with short birth spacing.
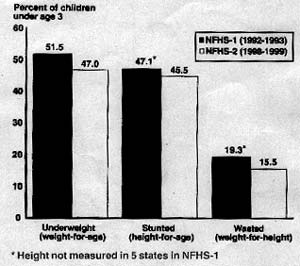
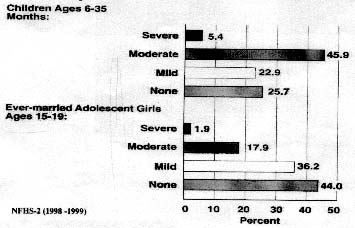
Morbidity and Mortality Among Children The common causes of illness are diarrheal disorders, respiratory infection and malnutrition for the last two decades - vaccine preventable diseases registering a decline. Severe malnutrition like kwashiorkar and blinding xerophthalmia have registered marked reduction. Still under nutrition is highly prevalent and between 40 to 50% of under fives are undernourished (Fig.1). Anemia is prevalent among all the population in developing countries. Various estimates reveal that the prevalence of anemia among different age groups varies from 50 to 90% (Fig.2).
Fig. 1. Undernutrition in children
Adolescent Population Twenty per cent of the population belongs to the adolescent age group. Ninety per cent of them are anemic. Undernutrition and stunting and other illnesses are highly pre-valent. They are victims of child labor, sexual assault and highly prone to drug addiction. Child population and women are victims of the silent emergency of malnutrition. Twenty to twenty five per cent of births still occur among adolescent girls resulting in a high incidence of complications and low birth weight Maternal Mortality Maternal mortality is a neglected tragedy and is prevalent among the poor with the least power and influence. India is one of the countries which has a very high MMR. According to SRS estimates, 1.1% of all deaths in the country in 1991 were due to maternal causes. Based on these numbers, the estimated maternal deaths are 0.63/1000 women in the reproductive age group of 14- 44 (MMR of 3.4/1000 live births). Obstetric complications like, bleeding of pregnancy and puerperium, abortion, toxemia, puer-perial sepsis and malposition are major causes. Non-obstetric causes particularly nutritional anemia account for more than 30% of maternal deaths. Recent observations have indicated that rheumatic heart disease contributed to 0.5 to 1% of maternal deaths indicating the need to institute aggressive preventive programs to prevent this condition. When a mother dies during pregnancy, the child has a 17 fold increased risk of dying during the first six months of life. There are wide variations between states - Bihar, Madhya Pradesh, Assam, Gujarat, Orissa, Uttar Pradesh have very high maternal mortality and childhood mortality rates. These are mainly due to female illiteracy, maternal malnutrition, inadequate obstetric care and bad socio-economic conditions. What Happened to Health for All by 2000 AD in India? For most villages and towns around the country and world, not much has changed for the better since 1978. Under five mortality, maternal mortality, incidence of low birth weight and under nutrition have not registered a substantial decline. The National Health Policy review is a review of broken promises (Table II). The Indian Government stated at Alma Ata "We are now laying greater emphasis on Primary Health Care in rural areas - on narrowing the gap between the village and the city and between the "health haves" and "have nots". The new direction which we have given to our health program seeks to take basic health care to the door steps of people in the village". These admirable sentiments and noble ideals were the solemn promises made by India. It implied removing the obstacles to health. What are the obstacles for achieving HFA goals?
Source: The National Health Policy, Sample Registration System 1993, 1998.
Reasons for Failure of Health for All
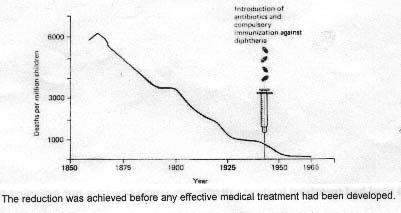
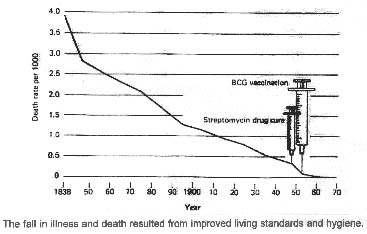
Disease and deaths in the developed countries in the not-too distant past were strikingly similar to that in most of under-developed world. Nutritional deficiency and infections played an important part in high death rates especially among children. In the developed world substantial reduction in deaths (85 to 90%) occurred before the era of antibiotics and vaccines by (i) Protected water supply; (ii) Proper sewage disposal; (iii) Improved food and nutrition; (iv) Provision of safe milk; (v) Improved living condition; (vi) Universal education. Decline in deaths was observed in air borne infections like diphtheria and respiratory infection (Fig. 3)(1). A rapid decline was also observed in water transmitted diseases (Fig. 4)(1) Tuber-culosis, traditionally considered to be a barometer of all aspects of health develop-ment registered a rapid decline long before advent of chemotherapy and BCG (Fig. 5)(1). Anti tubercular treatment has been available in India since 1944. India has a long and proud tradition in TB research and demonstration project since 1950. In fact most of the therapeutic strategies currently available and accepted globally have their roots in Indian research. Ironically, India has the saddest distinction of having the most cases of TB. The failure is due to dependence on drugs and medical care and not on health development.
Our Primary Health Care approaches failed to offer comprehensive health care. Many western donor institutions argued that comprehensive Primary Health Care is costly and unrealistic. To improve health statistics high risk groups were targeted with selective PHC approaches. This selective PHC stripped off its key concepts. This selective politically sanitized (and thus unthreatening) PHC was reduced to few high priority technological interventions like GOBI not determined by communities but by international health experts. This selective PHC was quietly embraced by national Governments. Health Ministries and many of the larger main stream international organizations. The failure is due to health being treated as a simple sector, the responsibility of health ministry and health professionals with the failure to involve all sectors with mass citizenship participation. Medicine of any sort plays a very minor role in improving the health of people as their health is inextricably linked to underdevelopment and the struggle against it. Despite the dismal and deteriorating living conditions in many poor counties, a few poor states have succeeded in making impressive strides in improving their people’s health - Kerala in India and Cuba(2). In spite of the economic backwardness, Kerala has made remarkable achievements almost comparable to that of developed countries, spending roughly about US$ 10 per capita per year within the frame work of constitution. US spends roughly $3500 per capita per year. Kerala has a highly literate population with high female literacy which has to be given due credit. Kerala has nurtured a political climate wherein the rights of the poor and the underprivileged have been upheld and fought for. There is remarkable reduction in the rate of exploitation of the underprivileged in Kerala compared to other Indian states. The public distribution system and universally available public health system has also contributed to the high health status of people.
Cuba, with a low per capita income (GNP) has a significantly lower U5MR. Not only are Cuba’s levels of health, education, and overall social welfare superior to any other ‘Third World’ country, but also in many ways they are equal, if not superior, to many of the Northern ‘developed’ countries. For immunization of children against measles and of pregnant women against neonatal tetanus, Cuba has the highest coverage rates in the world (98%). Cuba has also placed strong emphasis on equal rights of women. Cuba has managed, to date, to sustain the high levels of health of its children in spite of a 50% decline in its economy since the start of the 1990s. The two case studies indicate that non medical interventions play a major role in improving health.
The objective of medical education is primarily to support the development of the health of our nation, and hence it should be community-oriented. Unfortunately, our medical education is primarily hospital-based, specialization oriented and dependent on sophisticated investigatIVE procedures. The Edinburgh Declaration states "the aim of medical education is to produce doctors who will promote the health of all people". The Declaration suggested enlargement of the setting in which educational programs are conducted to include all health resources of the community, not hospital alone and to ensure that the curriculum content reflects the national health priorities and availability of affordable resources. It also emphasized the shift of training from passive to active learning. It is unfortunate that our medical education does not follow the spirit of the Edinburgh Declaration. What are the obstacles? To become a reality, Primary Health Care demands a number of funda-mental changes in medical society. Such profound changes do not come easily to the medical society, from a normal process of cumulative learning. They represent instead a revolution in thinking and living. The greatest resistance comes from the teachers themselves, both senior and junior, who do not want change. Teachers express concern that if community orientation gets priority, teaching has to be programmed beyond the four walls of hospitals and the medical colleges. They have also consider-able vested social, political and personal financial interest to resist any reform of the present system.
With Alma Ata declaration there has been a drastic expansion of community and health infrastructure, nutrition intervention and per-sonnel, spending a large amount of resources. An army of personnel in health and nutrition have received the necessary training for implementation of programs like CSSM and RCH and evaluation. Along with training equipments for essential newborn care, emergency obstetric and critical care were supplied in the last decade. In spite of all these inputs, there is no impact on maternal morbidity and mortality, high incidence of low birth weight and undernutrition. While government health centers exist across the length and breadth of the country, they have failed to provide the masses basic health care which the latter expect. A fairly large investment in public sector health care is wasted.
Medical education till recently was financed by the State. Until the last decade the private sector showed little interest and the entire burden of producing Doctors and Nurses was on the State. But in recent years Private Medical Colleges and Nursing schools are increasing in number rapidly without recognition by the Medical and Nursing council (Table III). This trend has been largely due to lack of any regulation on the growth of the private sector, and the large demand of doctors in mid-east and western countries. It must be noted that in spite of various restrictions, out migration of allopathic doctors remain very high with about 4000 to 5000 doctors leaving annually which in today’s price means a loss of Rs. 400 to 500 crores assuming Rs. 10 Lakhs as the cost of production of a doctor in public sector. Doctors under Homeopathy, Ayurvedic, Unani, Siddha, etc. are largely in the private sectors with very limited subsidy from the state. Even these doctors were largely produced for the private market. With the lack of any regulation of medical practice most of them indulge in wholesales cross practice, especially in Allopathy. In fact the Non Allopathic qualification is a via media for setting of the more profitable practice of medicine. The medical care in the private sector has witnessed a very rapid increase in the last decade and half making health care in accessible to the poor.
India has one of the most progressive patent laws passed by Parliament in 1970. The major feature of the patent laws being is that it is based on process patents rather than on product patents. It is because of Indian Patent that India has become one of the very few countries in the developing world that has attained near self sufficiency in essential drug production. The turnover of drugs is more than 16 thousand crores more than 90% of this being in the private sector. The private drug sector has penetrated into remote rural areas and has not deterred from using the large unqualified segment of practitioners to expand its market. For patients and consumers the major concern is the rapid increase in drug price making health services more expensive. With the rapid growth of medical equipment industry in India, the cost of medical care is increasing rapidly. The major impact of the WTO and TRIPS is in the pharmaceutical sector, destroying a self reliant pharmaceutical sector. MNCs push their drugs and equipment to the developing countries, making medical care very expensive and unreachable for the poor.
In the first half of this century, the image of the general practitioner was that of a family doctor and family friend who would come to homes, payment was flexible and often few drugs prescribed. Today, due to fierce competition private practice is: (i) threatened by numerous nursing homes and polyclinics; and (ii) swallowed up by corporate hospitals and insurance companies. For those who can not pay or are drained of their money, no treatment is offered. A very weak public sector fails to take care of the poor. A corporate hospital is run like an industry! It is run to maximize returns on investment. The number of people who need investigation will invariably be less than that needed to break even especially as more and more hospitals will open. Where there is a high return of investment in any sector in a market economy, more units of that type develop. Globalization has led to commercialization of medical care rapidly. The pressure to bring income by unethical means is very high in hospitals run for profit by non technical financiers. 7. Irrational Medical Care All types of irrational practices are rampant in India. The reasons are manifold. One is the proliferation of a large number of drugs in the Indian market that are either irrational or useless. With rapid developments in Science and Technology there has been an explosion in the number of drugs, which are available in the market. As a consequence there are an estimated 60,000 to 80,000 brands of various drugs available in the Indian market. On the other hand, the WHO lists a little over 270 drugs, which can take care of an overwhelming majority (over 95%) of the health problems of a country. A majority of the estimated 80,000 products in the market are either hazardous, irrational or useless. Another dangerous practice is that of making drugs available "over the counter", i.e., directly by chemists, without a doctor’s prescription. All irrational practices continue to flourish because the five actors in this drama: the government as a regulator, the drug companies as producers of drugs, the doctors as prescribers of drugs, the chemists as sellers of drugs, and the consumers as users of drugs, at some level or other do not fulfill the required obligations and are unmindful of the potential harm that inappropriate use of drugs can cause. Drugs can save lives, but their inappropriate use can also take lives. It is estimated that 20-30% of illnesses, especially in the aged and in children are caused by use of drugs. 8. Irrational Use of Diagnostics With irrational drug therapy as the basis, irrational use of diagnostics (including laboratory tests of blood, urine and sputum; X-rays; scans; etc.) may be defined as: "a diagnostic test is irrationally used when the expected benefit is negligible or nil or when it is not worth the potential harm or the cost". While there is some awareness about irrational drug usage, not enough attention has been focused on irrational use of diagnostics. If one realizes that irrational use of diagnostics - an irrational CT-scan is equivalent in wastage to about 100 bottles of an irrational ‘tonic’, then the importance of rational use of diagnostics will be apparent.
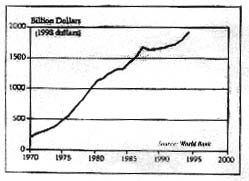
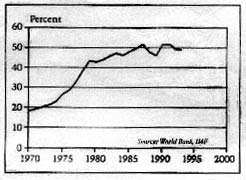
One should understand what globalization is all about and how it affects the health of the poor. In the British colonized India, the motivation beyond doubt was greed. Globalization is another form of colonialism. In the post World War period the rich became richer and were controlling the world economy. In 1973 the OPEC (Oil Producing Countries) suddenly hiked their price. This was followed by a long period of crisis in all the rich countries characterized by a slump in economic activity. There began an accumulation of money (or Capital - as economists call it) on an unprecedented scale in a few hands. A major source of this accumulation was due to the growing resources and influence of Multi National Corporations (MNCs) including infant food industry. Another source of accumulation was the huge profits made by oil producing countries, which they deposited into western capitalist banks. A third of capital accumulation was the increasing volumes of illicit or illegal incomes from crimes of various kind ranging from drug smuggling and drug peddling to the plunder (by dictatorial rulers and others from the ruling elite) of the wealth of developing countries. Thus, the availability of "surplus" money in the global economy became enormous, and it came at a stage when the economies of the developed countries were facing a slump and were incapable of absorbing this money in production related activities. This produced the impetus for the process of globalization, where avenues were sought, on one hand MNCs to sell their products in developing countries, and on the other by capitalist banks to push their money (in the form of loans) in developing countries. If both these objectives were to be met, the economies of the developing countries had to be prised open - to allow free flow of goods manufactured by MNC’s and to allow free flow of Capital from Western funding institutions. One glaring effect of globalization has been the explosive growth of MNC’s across national borders. Capitalism identifies nations, not as nations but, as "markets" and countries like India and China are the vast, untapped markets. As a global slump in productive activities creeps across the world, developed countries seek to expand their markets beyond their own boundaries and the obvious targets are nations such as India, even if the majority in these countries can barely make both ends meet. The objective of opening up Third World economies to the flow of capital was pursued relentlessly by two institutions set up by the Western capitalist countries after the Second World War-International Monetary Fund (IMF) and World Bank (WB). They claimed that their goal was to aid development! They directly control billions of dollars each year and indirectly even more. For the last 50 years the IMF and the WB have had unchecked decision making powers over managing the "Third World" debt. They have secured guaranteed flows of reserves from the South to the North. Since 1947 the WB has made profit every year. Between 1980 and 1992 its net earnings rose over 172% to over $1.6 billion. Both the IMF and WB are structurally undermocratic. Voting power does not operate on one vote for one country but is determined by the amount of money invested by each member country. While more than 150 countries are members of the IMF, five of them (USA, Britain, Germany, France, Japan and Saudi Arabia) control 44% of the votes. The USA alone controls 19% of the vote. In the case of the WB, the 24 OECD countries control more than two thirds of the votes. Clearly this gives the rich countries a great deal of power. Third World countries had been hit hard by the hike in oil prices in 1973. Further, in the 1970s developing countries faced increased economic problems as a result of unfair trade. Their economies were designed around the export of raw materials and agricultural products, the price of which was manipulated in the world market by developed countries. Over the last few decades the price of these commodities have declined sharply while the import of manufactured goods produced in the highly industrialized countries has increased. Faced with the twin crisis, the developing countries were eager to borrow more and more money from western banks, which, in turn, were only too happy to lend out more money and earn interest on their oil money. The crisis hit when the global economy slumped further and the interest rates for the money that was lent was hiked in the early 1980s. There were a number of other reasons for their falling into the debt trap like trade deficits and failure of development projects which were often a result of mismanagement and corruption! The ‘Third World’ debt currently (Figs. 6&7)(2) stands at approximately $1.3 trillion, which represent 44% of the combined Gross National Product of all so-called developing countries. India faced a debt crisis later than many other countries (in the late 1980s and 1990’s from the IMF and other foreign banks). This is Rs. 4,000 for each man, woman and child in India.
The ultimate result of the massive loans given by institutions like the World Bank and the IMF has been a massive loss of capital from the poor countries to the rich countries in the North - an estimated $50 billion in 1985 alone. In 1990 there was a net transfer of $156 billion from the "third world" to the developed countries. In other words, what is happening is, as a result of lending by the WB and the IMF, and the requirement to repay with interest, there is a reverse (Fig. 8)(4), flow from the developing countries to the developed countries, on a scale, which was unprecedented. The story does not stop here. In the face of the debt crisis banks and other financial institutions saw the need to safeguard their own interests, i.e., to ensure that they get back the money conditions were imposed on loans to "Third World" countries to ensure that there would be no defaulting on their debt repayments. Stringent conditions were imposed on further loans (Fig. 9)(4).
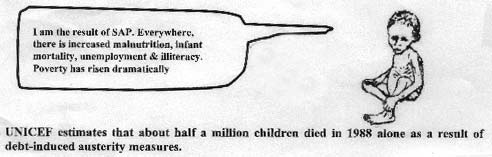
In brief, the Structural Adjustment Program (SAP) was designed to: (i) Cut government spending - this means big cuts in health care, education and subsidies to farmers and the poor; (ii) Privatize - state owned industries and services must be sold off to private interests. Often foreign multinationals are the buyers. Many workers lose their jobs as government industries close down. Services like transportation and power become more expensive; (iii) Devalue the local currency - for example, in India the rupee should be worth less and less compared to the American dollar. The World Bank and IMF demand this, so that what the country exports is cheaper in the international market to help to pay back the loans. But farmers and local industries get less for their goods. And prices of imports go up, increasing poverty; (iii) Export more-the country should export more to earn foreign dollars to pay back loans. The agricultural sector should turn to commercial farming for the market and for export, rather than food production for local consumption; (iv) Open up to foreign multinational companies like Pepsi, Shell Oil, Nike, Nestle, etc.; (v) Reduce duties and tariffs on imports - in this way foreign multinationals can more easily sell their products in a country like India. Local industries find it hard to compete with cheaper imports. Specifically in the health sector it meant
The Marginalized in the Present Scenario The policies have been disastrous for the third world. After SAP, maldistribution of global income has attained unacceptable levels. During the period 1960-70 the poorest 20% received 2.3% of the global income. In 1990 they received 1.3% of income - a reduction by half. While consumption has steadily increased in the industrial countries by about 2.3% annually over the past 25 years, the World’s poorest 20% live outside the consumption market. So globalization, WTO, SAP and others are making the poor poorer in both developed and developing countries. (Fig. 10)(2). The Role of Medical Profession to promote Health Development Pediatricians and physicians have to realize that they exist for serving the people, in whose satisfaction and welfare alone the profession can survive. They should have a functional code of ethics with accountability. They have a responsibility to address them-selves aggressively to the present and emerging problems. As teachers they have a responsibility to train medical graduates, professionals and others to make the delivery of health care more efficient and effective. It is time to reorganize themselves to take care of the community, the consumer, the patient and the people. They need to motivate students to work with new categories of health care providers and allied professional persons who can magnify and multiply the effectiveness of the work of pediatricians and physicians. They have to look beyond health sector and establish supportive linkages with education, health, agriculture, sanitation, communica-tion and comprehensive socio-economic development. They have to shift the main focus from drugs and doctors to informed practice by the people for health promotion and disease prevention. As administrators, pediatricians have to play a multifaceted role to promote health. They have to critically and objectively evaluate what is being done what can be done and what should be done in managing programs. Perceptions are changing in rela-tion to population growth. Lowering of birth rate cannot be separated from improving nutrition and health, education and socio-and economic improvement. They have to play a major role in influencing policy makers including fund controlling politicians, bureaucrats and program executives aggres-sively about marginalzing the poor with various new policies. They need to eliminate communication and information gap among all cadres of workers and community to facilitate community participation. The past century of the last millennium is called the century of the child, because paediatrics emerged as a medical speciality with increasing awareness that health problems differ from that of adults. The present century of the new millennium is a knowledge century with respect for human rights. The sense of human rights must be imbibed by us. We have to abide by all ethical principles. We have to respect not only the sanctity of life but also the quality of life.
References
|
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||