|
|
|
Indian Pediatr 2018;55:
997-998 |
 |
Bilateral Spontaneous
Urinoma in a Cyanotic Child
|
|
Swarnim Swarnim 1,
Dinesh Kumar1,
Dheeraj Bhatt1
and Sana Sana2
From 1Division of Paediatric Cardiology, Department of
Pediatrics, and Department of 2Radiodiagnosis; Post Graduate
Institute of Medical Education and Research and Dr Ram Manohar Lohia
Hospital, New Delhi, India.
Correspondence to: Dr Swarnim, Room No. 409, Doctors hostel, Ram
Manohar Lohia Hospital , New Delhi, India.
Email: [email protected]
Received: August 23, 2017;
Initial review: February 15, 2018;
Accepted: June 14, 2018.
|
Background: Urinoma is an encapsulated collection
of extravasated urine, secondary to trauma or obstructive uropathy.
Spontaneous bilateral urinoma is rare. Case characteristics:
7-year-old boy with cyanotic heart disease and fever of unknown origin.
Obeservation: The ultrasound abdomen and CT abdomen revealed
bilateral spontaneous urinoma which was aspirated and was found to be
infected. Following intravenous atibiotics the child became afebrile,
with subsequent renal scans showing no recurrence. Message:
Hypoxia and consequent polycythemia may be responsible for perinephric
leaks leading to Non-traumatic spontaneous urinoma.
Keywords: Cyanotic heart disease, Genitourinary system,
Perinephric collection.
|
|
U
rinoma is a collection of extravasated urine,
lying encapsulated in the perirenal space [1] – obstructive uropathy and
abdominal trauma are the commonly implicated causes. Bilateral
spontaneous urinoma is rare and uncommonly reported in literature. We
are reporting a case of bilateral spontaneous urinoma in the setting of
a cyanotic congenital heart disease in a child.
Case Report
A 7-year-old boy presented with bluish discoloration
of body since birth with history of squatting for the past 4 years. He
was admitted on account of worsening of cyanosis along with increased
frequency of cyanotic spells for the past two months. Examination
findings revealed central cyanosis with clubbing with a faint ejection
systolic murmur. Abdomen was soft with no organomegly. Other organ
systems were normal. Hemogram and biochemical workup were within normal
limits except for polycythemia. 2D echocardiography confirmed the
diagnosis of Double outlet right ventricle with pulmonary stenosis.
The patient was managed for cyanotic spells and
partial exchange transfusion was done for polycythemia. The patient
started having fever spikes following exchange for which broad spectrum
intravenous antibiotics were started. The hemogram showed raised counts
with neutrophilia; however, blood and urine cultures were sterile.
Urinalysis twice showed the presence of candida for
which intravenous liposomal amphotericin B was added. Despite treating
with broad spectrum antibiotics for more than a week the child continued
to have high spiking fever.
Widal Test, Malaria card test and peripheral blood
smear for malarial parasite, Weil felix test, Dengue and chikungunya
serology, Blood and urine culture, Urine for fungal hyphae, and Chest
X-ray were non-contributory. The ultrasound scan showed bilateral
loculated perinephric fluid collection with thin septa.
Contrast-enhanced computed tomography (EECI) scan of the abdomen with a
delayed phase was performed to rule out any causes of leak due to
obstructive uropathy like calculi, PUJ or VUJ obstruction. MCU was also
performed to rule out the presence of posterior urethric valve in the
patient.
From the perinephric area, 50 mL of pale yellow color
fluid resembling urine was aspirated under ultrasound guidance (Fig.
1). The biochemical analysis revealed that the fluid was comparable
to urine. The creatinine level in the fluid was 5 mg/dL (concurrent
serum sample 0.5 mg/dL). The glucose level was nil in the aspirated
fluid (serum glucose 95 mg/dL). A diagnosis of bilateral urinoma was
made.
 |
|
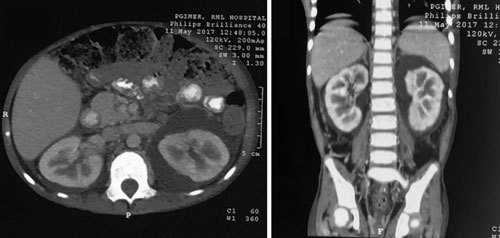
Fig. 1 Contrast CT (CECT) abdominal
scan showing bilateral perirenal fluid (white arrows) with
scalloping of left kidney (white arrow head), thickened
bilateral lateroconal fascia with pararenal fat stranding.
|
Microbiological analysis of the aspirated fluid
showed bacteria and 20 WBCs with cultures that were sterile. Intravenous
antibiotics were further administered for 14 days. Following
percutaneous aspiration of the infected fluid the child became afebrile
within 10 days. On serial renal ultrasound, small amount of perinephric
fluid was persisting and the child was asymptomatic. Subsequently, he
was discharged on oral antibiotics.
Discussion
Urinoma is an encapsulated collection of extravasated
urine in the perinephric space that leaks over a period of weeks into
the perirenal space [2]. It develops from disruption of the calices,
infundibuli or renal pelvis leading to leakage of urine in the
perinephric space, usually resulting from increase in intrapelvic
pressure following renal trauma, surgical procedures or obstructive
uropathy [3,4]. The fornices of the calyx are the usual site of leaks in
non-traumatic urinoma and the leak acts as a pop-off mechanism to
relieve intrapelvic pressure [5]. There are very few cases of
spontaneous perinephric urinoma in the literature. Rao, et al.
[6] described a 4-year-old boy with tetralogy of Fallot, who developed
bilateral spontaneous asymptomatic large urinoma [6]. The association of
severe cyanotic heart disease with polycythemia was postulated as the
pathogenesis [6].
The most likely other differentials in our case were
perirenal abscess and lymphangiectasia. In the absence of nephropathies
in our child the possibility of any post nephritic/nephrotic transudate
was ruled out. Although hematomas are usually common following trauma,
spontaneous non-traumatic hematomas may be associated with
angiomyolipoma, renal cell carcinoma, polycystic kidney disease, and
bleeding diathesis which were not present in our case. CECT scan is the
imaging of choice in perinephric hematoma. Ultrasound guided aspiration
of pus confirms its diagnosis. Renal lymphangiectasis is another rare
disorder which results from failure of renal lymphatic drainage into the
retroperitoneal lymphatics. Aspiration of chylous fluid confirms the
diagnosis [7]. CECT is the investigation of choice for the diagnosis of
urinoma. Urine leak on delayed excretory phase with fluid attenuation
confined to the perinephric space is confirmatory [7].
On percutaneous aspiration, fluid shows considerable
elevation of creatinine levels and decreased glucose levels relative to
serum levels in urinoma [3]. Since the urinoma was not causing any renal
compression it was managed with percutaneous ultrasound guided tap with
subsequent renal scans showing no recurrence.
Pediatricians need to be aware of this rare entity in
patients with predisposing conditions.
Contributors: Sw Sw, DK, DB: clinical management
of the patient; Sw Sw, Sa Sa: searched for literature and drafted the
manuscript; DK,DB: gave critical inputs and supervised the draft. The
manuscript was approved by all the authors.
Funding: None; Conflict of interest: None
stated.
References
1. Yang DM, Jung DH, Kim H, Kang JH, Kim SH, Kim JH,
et al. Retroperitoneal cystic masses: CT, clinical, and
pathologic findings and literature review. Radiographics.
2004;24:1353-65.
2. Brenner BM, Rector, Floyd C. In: Brenner
BM, editor. Brenner and Rector’s The Kidney. 8th ed. United States:
Saunders Elsevier, 2008. p.1476-8.
3. Titton RL, Gervais DA, Hahn PF, Harisinghani MG,
Arellano RS, Mueller PR. Urine leaks and urinomas: Diagnosis and
imaging-guided intervention. Radiographics. 2003;23:1133-47.
4. Chen SW, Shen ZJ, Yu YL, Zhou XL, Shi H, Liao GD,
et al. Subcapsular collection of glomerular filtrate: rare form
of page kidney. Nephrology. 2006;11:372-3.
5. Puri A, Bajpai M, Gupta AK. Bilateral spontaneous
perinephric urinomas: Case report and review of the literature. Urology.
2004;64:590-1.
6. Rao S, Vepakomma D, D’Cruz AJ. Bilateral
spontaneous asymptomatic urinoma: report of an unusual case. J Pediatr
Urol. 2007;3:507-8.
7. Sabale A, Pralhadan A, Kalidos K, Ramachandran K. Bilateral
perirenal space fibromatosis with renal infiltration: case report and
review of literature. Radiology Case Reports. 2016;11:438-43.
|
|
|
 |
|
