|
|
|
Indian Pediatr 2017;54:935-937 |
 |
A Prospective Study of
Homocysteine and its relation to Body Mass Index and Lipid
Profile in School Children
|
|
K Jagadish Kumar, Karen Saldanha, K Sushma, D
Srinivasa Murthy and *Prashanth Vishwanath
From Departments of Pediatrics and *Biochemistry, JSS
Medical College, JSS University, Mysore, Karnataka, India.
Correspondence to: Dr K Jagadish Kumar, 85/B, 9th
Cross, Navilu Road, Kuvempu Nagar, Mysore,
Karnataka 570 023, India.
Email: [email protected]
Received: November 19, 2016
Initial Review: April 07, 2017
Accepted: July 28, 2017.
Published online: August 24, 2017.
PII:S097475591600087
|
Objective: To study the serum Homocysteine levels
in children and its relation with body mass index (BMI), lipid profile
and plasma glucose. Methods: 138 children (age 5-15 y) were
enrolled and categorized into normal, overweight and obese group. Blood
homocysteine, lipid profile and plasma glucose were estimated.
Results: Out of 138 children, 46 (33%) were normal, 40 (29%) were
overweight and 52 (38%) were obese. Hyper-homocysteinemia was found in
34 (24.6%) of children. None of the normal children had
hyperhomocysteinemia in contrast to 15 (37.5%) in overweight and 19
(36.5%) in obese group (P=0.001).The median homocysteine levels
in obese and overweight children was significantly higher compared to
normal children (P=0.001).There was a positive correlation
between BMI and homocysteine levels. There was no significant
correlation between lipid profile and plasma glucose with homocysteine
levels. Conclusions: Serum homocysteine levels are significantly
higher in both overweight and obese children compared to normal
children.
Keywords: Metabolic, Obesity, Overweight, Risk factors.
|
|
The prevalence of childhood overweight and obesity, which is a major
risk factor for development of cardiovascular disease (CVD) at a younger
age, has shown rising trend in India [1]. Even moderate elevation of
homocysteine levels is shown to be associated with an increased risk of
CVD in children [2]. Four-fold increased risk for ischemic
cerebrovascular diseases is reported when serum homocysteine levels
exceed the 95th centile for age [3]. Serum homocysteine is considered as
one of the modifiable, independent risk factor for CVD in adults [4]. As
the risk begins early in life, estimation of homocysteine levels in
children offers an early opportunity for the primary prevention
[4,5]. This study aimed to determine homocysteine levels and its
relation with age, gender, body mass index (BMI) lipid profile and blood
sugar in obese and overweight children, and compare them with normal
children.
Methods
This is a cross-sectional study of 138 children
between the age group of 5 and 15 years conducted between August 2014
and December 2015 in a rural residential school of Mysuru, India.
Children on treatment with steroids, antipsychotics, anti-epileptics,
vitamin B12 or folic acid were excluded. The study was approved by the
JSS Institutional Ethical Committee and informed consent was obtained
from parents. Homocysteine levels, lipid profile and fasting plasma
glucose were estimated on automated analyzer (Randox Imola, BIO-02RX,
model OPT790DT).
Statistical analysis: Correlation was estimated
by Pearson product moment correlation. Comparison of categorical
variables was done by chi square test, or Fischer exact test. Mann
Whitney U test was used for comparison of medians.
Results
We studied a total of 138 children of whom, 46 (33%)
children were normal, 40 (29%) were overweight and 52 (38%) were obese
as per WHO BMI charts. The median homocysteine levels in obese
children and overweight children was significantly higher compared to
normal children (P<0.001). The median homocysteine level in girls
was higher as compared to boys (P=0.031) (Table I).
TABLE I Comparison of Homocysteine Levels (µmol/L) between Different Groups
|
Category |
Weight |
Age group |
Gender |
|
Parameter |
Normal |
Overweight |
Obese |
5 - 10 yrs |
11 - 15 yrs |
Male |
Female |
|
Number
|
46
|
40
|
52
|
66
|
72
|
91
|
47
|
|
Homocysteine level# |
7.3
|
16.7
|
16.6
|
13.7
|
12.9
|
11.8
|
15.6
|
|
(5.5-10.5) |
(11.2-22.5) |
(13.3-22.4) |
(10.3-19.7) |
(7.4-19.5) |
(7.7-19.0) |
(11.5-20.7) |
|
The median homocysteine levels in obese children and overweight children was significantly higher compared to normal children (P<0.001) and P=0.031 for comparison between boys and girls. |
Overall hyper-homocysteinemia was found in 34
children. None of the children in normal group had hyperhomocysteinemia
as compared to 15 (37.5%) in overweight group and 19 (36.5%) in obese
group (P<0.001). There was no gender difference in the prevalence
of hyper-homocysteinemia (Table II).
TABLE II Proportion of Hyperhomocysteinemia in Various Groups
|
Normal |
Over weight |
Obese
|
Male |
Female |
|
Normal Homocysteine |
46 (100%) |
25 (62.5%) |
33 (63.4%) |
70 (%) |
34 (%) |
|
Hyper homocysteinemia* |
0 (0.0) |
15 (37.5%) |
19 (36.5%) |
21 (%) |
13 (%) |
|
*Serum Homocysteine value >20 µmol/L; P<0.001 for comparison
between normal and overweight, and between normal and obese. |
The homocysteine levels in children between the age
of 5 and 10 years and children between 11 and 15 years were not
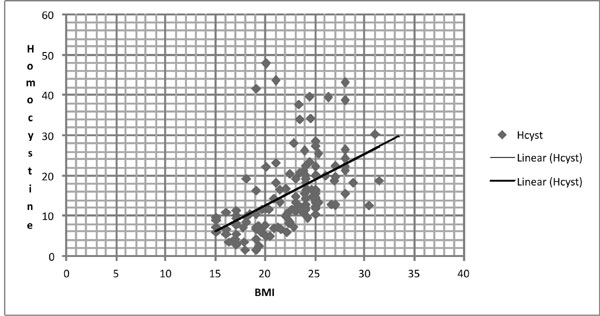
significantly different (Table I). There was a positive
correlation between BMI and homocysteine levels (Fig. 1).
There was no statistically significant correlation between lipid profile
and plasma glucose with homocysteine levels.
 |
|
Fig. 1 Correlation between BMI and
Homocysteine Levels
|
Discussion
This study showed a strong association of
homocysteine levels with obesity and overweight in school children. This
suggests that the risk of cardiovascular disease may increase as the BMI
increases, even before obesity sets in. Closer to one-third of
overweight and obese children were observed to have hyperhomocysteinemia,
whereas none of the normal weight children had hyper-homocysteinemia.
The major limitation of the study was that we did not
assess the vitamin B12 and folate levels, which are well known to
influence homocysteine levels. Other limitations are convenience
sampling, small sample size and non-assessment of functional outcomes
related to hyper-homocysteinemia.
The significant difference in homocysteine levels
between overweight and obese children when compared to normal children
in our study is similar to observations made from various countries
[6,7]. In contrast, few other studies have found no significant
difference between obese, overweight and normal children with respect to
hyperhomocystenimia [8,9]. Genetic and ethnic factors playing role in
the homocysteine homeostasis is indicated in several reports where
higher concentrations of homocysteine in immigrant ethnic Indian adults
compared to North Americans and European whites [10,11]. This could have
contributed for the difference in the results noted in our study and
that of others.
Our observation of significant positive correlation
between homocysteine levels and BMI is similar to few other studies from
various countries [2,3,6,10,12]. We did not find any statistically
significant correlation between homocysteine levels and lipid profile
similar to other studies [4,12]. Huemer, et al. [3] showed that
homocysteine concentration correlated positively with triglycerides but
not cholesterol. The variations of homocysteine levels and its
correlation with other risk factors among various studies may be due to
the fact that many factors like ethnicity, age, gender and nutritional
status affects homocysteine metabolism and its serum concentrations.
To conclude, serum homocysteine levels are
significantly higher in both overweight and obese children compared to
normal children. Currently, obesity is considered as disease and
overweight is not. This approach need to be relooked in order to pick
children at-risk at the earliest.
Acknowledgements: Dr D Narayanappa, Head of the
Pediatric Department, Dr Ravi, Vice Pricipal, and Dr Basavanagowdappa,
Principal of JSS Medical college, for their constant support and
encouragement.
Contributors: KJ: conceived the research
question, contributed to the study design, and helped in preparing the
manuscript. KS: collected the data, did the literature search and
contributed for analysis of data and preparation of the manuscript; SMD:
helped in study design, analyzing the data and preparing the manuscript;
SK: helped in literature search, analysis of data and preparing the
manuscript; PV: conceived the research question, contributed for the
study design, analysis of the samples and data. All the authors have
approved the final version of manuscript.
Funding: None; Competing interest: None
stated.
|
What This Study Adds?
•
Serum homocysteine levels and
the prevalence of hyperhomocystenemia in overweight children is
similar to that seen in obese children suggesting that the risk
may increase as the BMI increases even before obesity sets in.
|
References
1. Jagadesan S, Harish R, Miranda P, Unnikrishnan R,
Anjana RM, Mohan V, et al. Prevalence of overweight and obesity
among school children and adolescents in Chennai. Indian Pediatr.
2014;51:544-9.
2. Papandreou D, Mavromichalis I, Makedou A, Rousso
I, Arvanitidou M. Total serum homocysteine, folate and vitamin B12 in a
Greek school age population. Clin Nutr. 2006;25:797-802.
3. Huemer M, Vonblon K, Fodinger M, Krumpholz R, Hubmann
M, Ulmer H, et al. Total homocysteine, folate, and cobalamine,
and their relation to genetic polymorphisms, lifestyle and body mass
index in healthy children and adolescents. Pediatr Res. 2006;60:764-9.
4. Osganian SK, Stampfer MJ, Speigelman D, Rimm E,
Cutler JA, Feldman HA, et al. Distribution of and factors
associated with serum homocysteine levels in children. JAMA.
1999;281:1189-96.
5. Greenlund KJ, Srinivasan SR, Xu J, Dalteres E Jr,
Myers L, Pickoff A, et al. Plasma homocysteine
distribution and its association with parental history of coronary
artery disease in black and white children. The Bogalusa Heart Study.
Circulation. 1999;99:2144-9.
6. Abaci A, Akelma AZ, Ozdemir O, Hizli S, Razi CH,
Akin KO. Relation of total homocysteine level with metabolic and
anthropometric variables in obese children and adolescents. Turk J Med
Sci. 2012;42:69-76.
7. Kandil ME, Anwar GM, Fatouh A, Salama N, Ahmed A,
Elabd E, et al. Relation between serum homocysteine and carotid
intima-media thickness in obese egyptian children. J Clin Basic Cardiol.
2010;13:8-11.
8. Brasileiro RS, Escrivao MA, Taddei JA, D’Almeida
V, AnconaLopez F, Carvalhaes JT. Plasma total homocysteine in Brazilian
overweight and non-overweight adolescents: A case-control study. Nutr
Hosp. 2005;20:313-9.
9. Papandreou D, Rousso I, Makedou A, Arvanitidou M,
Mavromichalis I. Association of blood pressure, obesity and serum
homocysteine levels in healthy children. Acta Paediatr. 2007;
96:1819-23.
10. Anand P, Awasthi S, Mahdi A ,Tiwari M, Agarwal
GG. Serum homocysteine in Indian adolescents. Indian J Pediatr.
2009;76:705-9.
11. Chambers JC, Obeid OA, Refsum H, Ueland
P, Hackett D, Hooper J, et al. Plasma homocysteine concentrations
and risk of coronary heart disease in UK Indian Asian and European men.
Lancet. 2000;355:523-7.
12. Shen MH, Chu NF, Wu DM, Chang JB. Plasma
homocyst(e)ine, folate and vitamin B(12) levels among school children in
Taiwan: The Taipei Children Heart Study. Clin Biochem. 2002;35:495-8.
|
|
|
 |
|
