Pneumonitis develops in 15-25 % of Cytomegalovirus (CMV) infected
preterm infants [1]. There are occasional case reports of congenital
lobar emphysema and Wilson- Mikity syndrome in CMV-infected neonates
[2,3]. We report a CMV-infected preterm neonate who developed a cystic
lung disease.
A preterm (31 weeks) girl delivered by Caesarean
section with a birth weight of 1060 g to a primigravid mother was on
full feeds (with expressed breast milk) by day-8 of life. On day-23 of
life, child developed respiratory distress and apnea, and was started on
antibiotics and oxygen. X-ray showed a left lower zone
consolidation. Blood culture showed no growth and intravenous
antibiotics were given for 7 days. She required supplemental oxygen for
14 days. As the baby recovered, X-ray showed clearing of the
consolidation with appearance of bubbly lucencies, and the left dome of
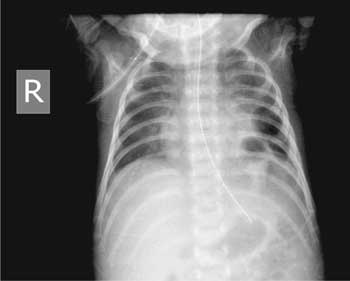
the diaphragm was not well visualized. The lesions then coalesced into a
few well-defined cysts (Fig. 1). Urine PCR for CMV was
positive as also the serum CMV IgM. Baby’s hearing screen and eye
examination were normal. By two weeks, baby had no respiratory distress.
She was discharged 4 weeks later. She is currently 2-year-old and is
developmentally normal. Serial X-rays were done and one at 9
months showed complete resolution of the cysts.
 |
|
Fig. 1 Cystic lucencies in lower zone
of left lung in a CMV-infected neonate.
|
Our patient was asymptomatic at birth and initial
chest X-ray was normal. The absence of cysts on the first X-ray
was in favor of an acquired rather than congenital lung cyst. Even
though it is difficult to prove causation, we did not find another
explanation for the lung cyst other than CMV infection in this baby.
Since the CMV PCR was not done within the first week, we could not
definitely say if the CMV was acquired transplacentally or perinatally.
The association between lung cysts and acquired CMV infection has been
reported earlier [4]. Carrol, et al. [2] described association of
congenital lobar emphysema and CMV infection in a 32 weeks gestation
preterm neonate [2]. We recommend that CMV infection should be
considered as differential diagnosis in the newborns presenting with
acquired lung cysts.
Contributors: MK: carried out the literature
review and drafted the manuscript. He was also responsible for the
diagnosis and management. SS: reviewed the manuscript.
Funding: None; Competing interests: None
stated.
References
1. Coclite E, Di Natale C, Nigro G. Congenital and
perinatal cytomegalovirus lung infection. J Matern Fetal Neonatal Med.
2013;26:1671-5.
2. Carrol ED, Campbell ME, Shaw BN, Pilling DW.
Congenital lobar emphysema in congenital cytomegalovirus infection.
Pediatr Radiol. 1996;26:900-2.
3. Reiterer F, Dornbusch HJ, Urlesberger B, Reittner
P, Fotter R, Zach M, et al. Cytomegalovirus associated neonatal
pneumonia and Wilson-Mikity syndrome: A causal relationship? Eur Respir
J. 1999;13:460-2.
4. Bradshaw JH, Moore PPC. Perinatal cytomegalovirus
infection associated with lung cysts. J Paediatr Child Health.
2003;39:563-6.


