|
|
Research Papers Indian Pediatrics 2008; 45: 899-904 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Intravenous Ketamine plus Midazolam vs. Intravenous Ketamine for Sedation in Lumbar Puncture: A Randomized Controlled Trial |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
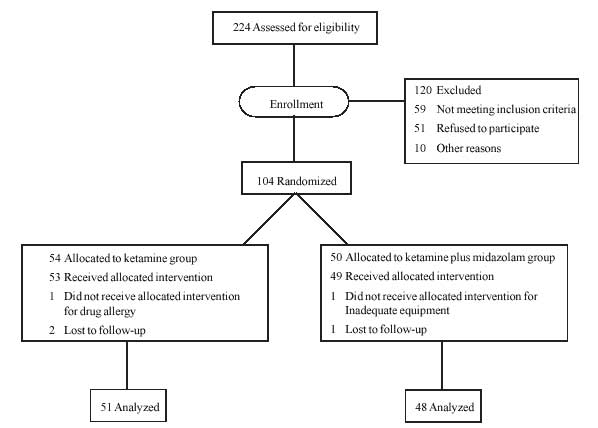
Introduction Providing procedural sedation and analgesia to patients to accomplish painful procedures is becoming a standard practice in every emergency department. The ideal agent for sedation for a brief painful procedure must be safe and easy to administer, provide adequate amnesia, and have a rapid onset and recovery time. Ketamine is commonly used for sedating children during medical procedures. This drug can induce dreaming, hallucinations, and unpleasant reactions as nightmares during recovery. Benzodiazepines are frequently administered with ketamine with the intent of preventing or reducing recovery reactions. According to the recommendations of American Society of Anesthesiologists (ASA) combinations of sedative and analgesic agents may be administered; each component should be administered individually to achieve the desired effect (e.g. additional analgesic medication to relieve pain; additional sedative medication to decrease awareness or anxiety) and sufficient time must elapse between doses to allow the effect of each dose to be assessed before subsequent drug administration(1). Midazolam plus ketamine has been used in adults, however data on the use of this combination is lacking in children, during lumbar puncture(2,3). We aimed to compare ketamine versus ketamine plus midazolam sedation in terms of efficacy and safety when used for sedation during lumbar puncture in children. This was a prospective clinical study conducted in the Pediatric Emergency Department (PED) at Ankara Training and Research Hospital, Ministry of Health, Turkey. Methods We included 99 children (age, 2-14 years) requiring lumbar puncture for suspected meningitis, admitted between January 2004 and December 2006. Children were eligible for the study if they were hemodynamically and neurologically stable. Children with a history of an adverse reaction to midazolam or ketamine, psychiatric or behavioral disorder, risk of raised intracranial or intraocular pressure, thyroid disorder, porphyria, blocked nose, or who had been sedated within 4 h of presentation were excluded. The study was explained to the patient and caretakers and written informed consent was obtained. An approval from the Institutional Ethical Committee was also obtained for the study. Randomization: Subjects were randomly assigned using computer-generated randomized allocations sealed in opaque envelopes. Study physicians responsible for recording the child’s procedural sedation analgesia form were not present during drug administration and were unaware of each subject’s allocation. Intervention: Intravenous (IV) ketamine and midazolam were used for procedural sedation analgesia. After receiving a dose of atropine as an antisialogogue (0.01 mg/kg; 0.1 mg minimum and 0.5 mg maximum), IV ketamine was administered at a dose of 1 mg/kg (100 mg/mL solution diluted to 10 mg/mL in 0.9% saline; IVK group) as a slow IV push over 1 min. In the IVKM group, IV midazolam was administered slowly over 1-2 min at a dose of 0.1 mg/kg (5 mg/mL solution diluted to 1 mg/mL in 0.9% saline), and IV ketamine was administered at a dose of 1 mg/kg. We added 0.5 mg/kg ketamine if conscious sedation was not achieved within 5 min during the procedure. In the IVKM group, none of the patients needed an additional dose of ketamine, whereas it was administered twice in five patients in the IVK group. The procedure was started when the senior study physician noted sufficient sedation of the patient. While the senior physician was performing the procedure, a procedural sedation analgesia form was recorded by the assistant physician. All subjects were evaluated by the same physician. We used a bedside monitor for respiratory and heart rates. Oxygen saturation was measured with a pulse oximeter. These parameters were recorded on the procedural sedation analgesia forms at 5-min intervals, beginning before drug injection and ending after the procedure when the patient was fully awake. Outcome measures: Fasting time was noted as the last meal time to the time of the first dose of medication. Time to sedation was defined as the time from administration of the first drug to when the patient was consciously sedated. Recovery time was defined as the time that elapsed from when the last dose of medication was given to when the patient returned to his or her baseline sensorium. Patients were discharged 2 h after the procedure, after ensuring that they were fully awake, coherent, and able to tolerate oral food. Apnea was defined as cessation of respiration for >20s. Desaturation was defined as any time during which a patient’s oxygen saturation was <90%. Hypotension was defined as a systolic blood pressure below the 5th percentile of normal for the patient’s age. Nightmares were identified when children described unpleasant visual imagery. After recovery, amnesia and analgesia were evaluated with yes/no questions; the children were asked if they remembered the procedure and if they felt pain after the procedure. Late complications following discharge were recorded in a subsequent telephonic follow-up 3 weeks after the procedure. Parents were asked yes/no questions about the occurrence of dizziness, nausea/vomiting, and nightmares/crying spells. Additionally, parental satisfaction ratings with the sedation process were noted as unsatisfied, satisfied, or very satisfied. Statistical Analysis: Dichotomous variables, were analyzed using the chi-square test. Comparisons between the groups were analyzed using a two-tailed Student’s t-test for independent samples or the Mann-Whitney U test. The Spearman rank test was used to analyze the relationship between fasting time and nausea/vomiting. The relationship between dependent and independent variables was evaluated by logistic regression analysis. All analyses were performed using (SPSS, version 13.0). A P value of 0.05 was deemed statistically significant. Results Demographic and clinical characteristics of the patients are shown in Table I. The overall incidence of adverse events was not different between the IVK (n=23, 45.1%) and IVKM groups (n=20; P=0.88). There was no association between fasting time and any adverse events (OR: 0.39, 95% CI: 0.8-1.0; P= 0.94). Desaturation was not observed in the IVK group, whereas three patients (6.3%) in the IVKM group required supplemental oxygen (P=0.11). Dizziness was reported by 10 patients (20.8%) in the IVKM group and 5 patients (9.8%) in the IVK group (P=0.16). In the IVKM group, a single episode of hypotension (2.1%) occurred in a 3 year-old, 12-kg boy during the lumbar puncture procedure; hypotension was not noted in any patient in the IVK group (P=0.18). Nausea/vomiting was more frequent in the IVK group (n=14, 27.5%) than in the IVKM group (n=7, 14.6%; P=0.08). Fasting time did not correlate with nausea/vomiting (P=0.80, r=0.02). Nightmares/crying spells were more common in the IVK group (n=10, 19.6%) than in the IVKM group (n=3, 6.3%; P=0.04). An age breakdown showed 33.4% more episodes of nausea/vomiting in children >5 years and 38.4% more episodes of nightmares/crying spells in children <5 years in both groups, although these were not statistically significant (P= 0.22 and P=0.08, respectively). All patients (n=48) in the IVKM group and 41 (80.3%) patients in the IVK group had complete amnesia regarding the procedure (P=0.001). Two patients (4.2%) complained of post-procedural pain in the IVKM group, whereas 5 patients (9.8%) reported pain after the procedure in the IVK group (P=0.24). Parental satisfaction was significantly higher in the IVKM than the IVK group (P=0.001). Table I Demographic and Clinical Characteristics of Children in the Two Groups
*Intravenous ketamine group, **Intravenous ketamine plus midazolam group During the telephone follow-up interview 3 weeks after the initial PED visit, 78.6% of the subjects were reached; no adverse event was reported in IVK group, whereas one nightmare complaint (1.9%) was noted in the IVKM group (P=0.51). Discussion We compared ketamine alone and ketamine plus midazolam sedation in terms of efficacy and adverse events in children undergoing lumbar punctures for suspected meningitis. Our study demonstrated that although the sedation time in the IVK group was longer than that in the IVKM group, overall adverse events were not significantly different between the groups. Although nausea/vomiting and nightmares/crying spells were significantly more in the IVK group, desaturation and hypotension occurred more frequently in IVKM group, although not statistically significant.
Though lumbar puncture is well described in pediatric textbooks, the use of anesthetics for this procedure remains controversial(4,5). Adequate use of analgesia during this painful procedure is limited(6,7). Friedman, et al.(8) demonstrated that midazolam decreased pain and anxiety related behaviors in children before and after lumbar puncture. We also observed that parental satisfaction was higher when midazolam was combined with ketamine. Currently, the combination of ketamine and midazolam is widely used for sedation in pediatric populations(9-14). In a pediatric study, it was reported that adding midazolam to ketamine sedation reduced the incidence of emergence phenomena(12). In the present study nightmares/crying spells were less common in the IVKM group. In another study, Wathen, et al.(15) studied 266 children and reported that the addition of midazolam did not alter the incidence of adverse events. Similarly, we found that the incidence of overall adverse events did not differ between groups. Wathen, et al.(15) also reported no difference in the length of time of sedation between groups of patients receiving ketamine versus ketamine plus midazolam. We found that the time to sedation was significantly shorter in the IVKM group compared to the IVK group. Given the lack of evidence, supplemental oxygen is not required in all patients and is used at the physician’s discretion(16). We did not use supplemental oxygen in any of the 99 patients and observed transient desaturation in only three patients. Agrawal, et al.(17) reported that there was no difference in the incidence of adverse events, especially vomiting, among fasting and non-fasting sedated patients. We also observed that the incidence of adverse events such as vomiting did not appear to be associated with fasting time. Newman, et al.(18) studied 1341 sedation events over a 2-year period to determine the optimal time of discharge following procedural sedation analgesia and concluded that patients could be safely discharged 30 min after final sedation medication administration if no adverse event had occurred by then. Our patients were discharged 2 h after the procedure. With ketamine sedation, adverse effects can occur up to 3 weeks after the sedation(19). Although we contacted 78.6% of the enrolled patients via telephone for a follow-up interview, the inability to contact all patients may have resulted in under-reporting of the total number of adverse events. Our study had several limitations. The decision to use a convenience sample was based on the availability of the two principal investigators. Patient recruitment was also in the context of a busy PED. However, we believe that our results closely reflect the nature of clinical practice in our busy urban pediatric PED. Another potential limitation was that we did not objectively measure the depth of sedation. However, all subjects were evaluated by the same physicians. Contributors: DD was responsible for the concept and study design. DD and NHS were involved in collection, analysis and interpretation of data. DD drafted the manuscript, which was critically reviewed and approved finally by YD and DD. Funding: None. Competing interests: None stated.
|
![]()