|
|
Research Papers Indian Pediatrics 2008; 45:893-898 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Role of Chest X-ray in Predicting Outcome of Acute Severe Pneumonia |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Bhavneet Bharti, Ladbans Kaur and Sahul Bharti From Civil Hospital, Rohru, Shimla, Himachal Pradesh, India. Correspondence to : Dr Bhavneet Bharti, Assistant Professor, Advanced Pediatric Center, Postgraduate Institute of Medical Education and Research, Chandigarh 160 012, India. E-mail: [email protected] Manuscript received: July 18, 2007; Initial review
completed: October 1, 2007;
Introduction Traditionally, guidelines classify children with pneumonia into phenotypic subtypes based mainly on the distribution of tachypnea and lower chest indrawing in a community setting(1). Nonetheless, radiological evaluation is invariably at the forefront when a clinician encounters a child with suspected pneumonia in the hospital. Most of the radiological studies in pneumonia have focused on epide-miologic, diagnostic and etiological perspectives. The evaluation of clinical outcome measures (time to defervescence of fever and tachypnea) has been infrequently taken into account vis-à-vis underlying type of radiological abnormalities(2-4). Given the paucity of data about clinical-radiological interface of pneumonia in resource constrained settings, this study aimed to identify easily observable respiratory features or patient characteristics that were associated with radiological abnormalities and, to evaluate the role of chest radiography in determining the clinical outcome (time to defervescence) of acute severe pneumonia. Methods All consecutive children, mostly 5 years or below, hospitalized with severe pneumonia were prospectively evaluated throughout their length of stay in hospital. Children having duration of illness >2 weeks or predominant wheezing were excluded. Patients were enrolled between May 1997 and June 1998 at a Civil Hospital (Tehsil Rohru, district Shimla) serving a catchment area of approximately 100 villages in Himachal Pradesh, India and caring for 200 to 300 patients per day (with pediatric patients constituting at least 1/3rd of daily outpatient attendance). The diagnosis of severe pneumonia was based on either WHO criteria for children aged 5 years or less(1) or typical auscultatory signs of pneumonia in older children (only 5 patients). All children were subjected to chest radiography if feasible. Nutritional status was expressed as z scores for weight-for-age using reference median values of healthy Indian children. Clinical evidence of rickets was recorded if at least two of the following criteria were found: widening of wrists, rachitic rosary, box shaped head with frontal bossing, pectus deformity of chest, and abnormally wide or open anterior fontanel. Two clinical researchers recorded the history and physical findings, clinical course and resolution of symptoms and signs throughout the length of stay in hospital. An experienced radiologist, unaware of clinical findings, reported on all the chest radiographs. The three mutually exclusive radiographic groups were defined as follows: (i) unequivocal focal or segmental consolidation with or without pleural effusion; (ii) interstitial pneumonia with diffuse bronchovascular markings with or without hilar lymphadenopathy; and (iii) normal chest radiographs. Descriptive and graphic analyses were used to analyze means, standard deviations, and normality of data. Non parametric tests (Mann Whitney U test and Kruskal Wallis test) for quantitative data, and Chi-square and Fisher exact test for categorical data were used. Results 115 consecutive children, aged 2 months to 10 years, hospitalized with severe pneumonia were pros-pectively evaluated. Radiographic investigation could be carried out only in 90 children. Seven chest radiographs were further excluded from this study (4 suboptimal and 3 wrongly labeled). The mean (+SD) age of remaining 83 children was 1.9(±1.6) years (median age 1.25 years, range 3 months to 7.3 years); 43(51.3%) were male. Chest radiographs were reported as normal in 14(16.9%); lobar consolidation was observed in 43(51.8%) including one empyema and two small pleural effusions; and 26(31.4%) had interstitial pneumonia with diffuse and prominent bronchovascular markings. Perihilar prominence and/or hilar lymphadenopathy occurred in 20(24.1%) cases. Three children with consolidation had typical air bronchogram patterns and one infant presented with hyperinflation as well. The lobar consolidation (n=43) occurred on right side in 26(60.5%), left side in 9(20.9%) while remaining 8(18.6%) children had bilateral consolidation. Similarly, of 26 children with interstitial abnormalities on chest radiographs, 18(69.2%) had diffuse bilateral picture, 2(7.7%) with predominantly left side involved while remaining 6(23.1%) had predominantly right-sided involvement. TABLE I Demographic Variables, and Symptoms and Signs of Respiratory Illness in Children with Severe Pneumonia Stratified by their Chest X-ray Findings
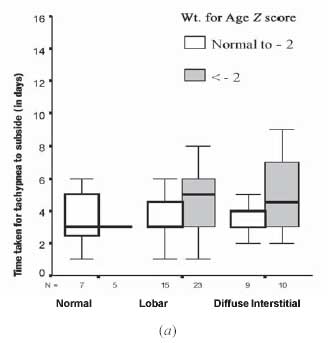
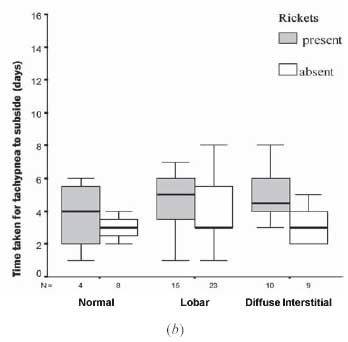
When demographic and clinical characteristics of children with severe pneumonia were stratified by their groups of radiographic findings (normal, lobar consolidation and interstitial pneumonia), no significant differences were observed for the various characteristics among different radiographic groups (Table I). There was only a trend for significance in the occurrence of normal chest radiographs in infants (10/39, 25.6%) as compared to children above one year of age (4/44, 9.3%) (P=0.07). Of the remaining 29 infants with severe pneumonia, 18 (46.2%) had consolidation while 11(28.2%) had interstitial radiographic abnormalities. Duration of illness after onset of respiratory symptoms till hospitalization was not significantly different between those with normal and abnormal chest radiographs. However, those with lobar consolidation showed a marginal trend in presenting earlier (5.2±2.2 days) than those with interstitial radiographic findings (6.7 ±3.8 days) (P=0.07). Moreover clinical character-istics and outcome measures did not differ statistically between right sided (n=26) vs. left sided (n=9) lobar consolidation. Chest radiographic findings were further analyzed on the basis of vaccination status in affected children. A completely vaccinated child in current study received only conventional vaccines that are routinely provided in a primary health care setup. None of the vaccinated children received newer vaccines for H. influenzae or Pneumococcus. Out of 28 children with nil or incomplete vaccination status, 67.9% had lobar consolidation and 14.3% had diffuse interstitial pneumonia. In contrast, only 43.6% of completely vaccinated children had lobar consolidation while 40% had diffuse interstitial pneumonia (P=0.04). The radiological findings also lacked any statistical relationship with various clinical outcome measures (Table II). On the other hand, clinical signs of severe pneumonia were significantly related to outcome measure of tachypnea defervescence after start of therapy. Mean duration of tachypnea to subside after admission was significantly longer in those children with severe tachypnea at admission (Spearman correlation r=0.48, P<0.001), severe lower chest indrawing (P=0.03), and grunting (P=0.03). Radiographic abnormalities showed significant univariate association with length of hospital stay (Table II). Malnutrition prevalence was high in our study cohort; 57% children having weight for age below –2 Z score (based on median references of Indian Children) and rickets affected slightly less than half of (43.4%) enrolled children. Defervescence of tachypnea demonstrated a trend for delayed resolution in children with weight for age Z score below –2 (P=0.05) as well as presence of rickets (P=0.06). This was more pronounced in children with abnormal chest radiographs (Fig. 1 a,b). TABLE II Clinical Outcome Measures Stratified by Chest Radiographic Findings
* Duration of hospitalization when the variable occured; †CXR (chest radiograph) 1 = normal, 2 = lobar consolidation, 3= diffuse interstitial; ** Only children with complete follow up data were included for analysis
Discussion Chest radiography has carved a vital and inevitable niche in the management of childhood pneumonia, particularly in developed countries. Though opti-mized for epidemiological use, radiographic reference standards in pediatric pulmonary infections are yet nebulous for use in direct clinical care(5-7). Moreover, little is known about the link between key radiological attributes to clinical defervescence outcomes in childhood pneumonia in resource constrained settings(2,8). The current study, therefore, is one such study conducted in hospitalized children with severe pneumonia detailing underlying radiological features and their association with clinical measures of defervescence. Our analysis highlights the premise that radiological landscape in pneumonia tends to have either extreme features to guide their clinicians (e.g. empyema or lobar consolidation with air bronchogram and effusion), or "completely masquerade radiologists" (with seemingly normal chest radiographs)(8-11). A well-defined lobar consolidation in 51.8% of cases in our study is an overarching indicator of severity of pneumonia and possible bacterial etiology(12-14). This finding is further supported by a review of 59 studies where a bacterial cause was confirmed in over 50% of cases by lung tap(15). Still, normality of chest radiographs in 16.9% of children with severe pneumonia leaves one second-guessing about their "rule in" utility, particularly in infants. Infants accounted for 71.4% of normal chest radiographs (10/14) in our study cohort. Anecdotal evidence suggests this as typical of early phase of pneumonia presenting with fever and tachypnoea before chest radiographic changes are seen(9,16). Moreover, the abnormal radiological appearance is often difficult to define especially in infants with inflammatory lung illness where hyperinflation may be the only radiological clue and features of the airspace consolidation are lacking(17). Another interesting observation in our study was the higher distribution of radiological consolidation in non vaccinated or incompletely vaccinated children (68%) as compared to completely vaccinated children (44%), though the two vaccination groups did not vary in other confounding factors like malnutrition, rickets as well as severity of respiratory illness. There is already some epidemiological evidence of heterologous immunity and nonspecific protective effects of live vaccines against non-targeted infections particularly in high mortality areas(18). The time to defervescence of fever and tachypnea did not differ depending on the type of underlying radiological findings in our study, though children with lobar consolidation and possibly bacterial etiology had significantly longer duration of hospital stay in our study. This is in contrast to the results of a study by Lin, et al.(19) where fever clearance took much longer duration in complicated lobar pneumonia as compared to uncomplicated lobar consolidation in children. This clinical recovery-radiological dissociation may however be due to lack of complicated lobar pneumonia cases in our study. As regards the utility of chest radiographs, a randomized controlled trial by Swingler, et al.(20) had not favored the routine use of chest radiographs in ambulatory children aged over 2 months with acute lower respiratory infections when stratified further by WHO case definition of pneumonia. Similarly, our cohort study also echoes the inadequacy of radiological inputs in the recovery outcomes measures of hospitalized children with severe pneumonia and further endorses the WHO case management guidelines of using simple clinical signs to manage pneumonia in children in resource constrained settings, in developing countries. We, however, consider that some caution is required before using our results in different settings especially due to lack of mortality and fewer complicated pneumonia cases in our study. Furthermore, the interpretation of chest radiographs by single radiologist could be another limitation of our study. Contributors: BB was involved in designing the study and she will act as guarantor of the study. BB and SB were involved in data collection, analysis and manuscript writing. LK analyzed and interpreted the radiological data. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()