|
|
Case Reports Indian Pediatrics 2007; 44:854-856 |
|||||
|
Oral-Facial-Digital Syndrome Type 1 |
|||||
|
Ercan Mihci
Manuscript received: December 27, 2006; Initial review
completed: February 6, 2007;
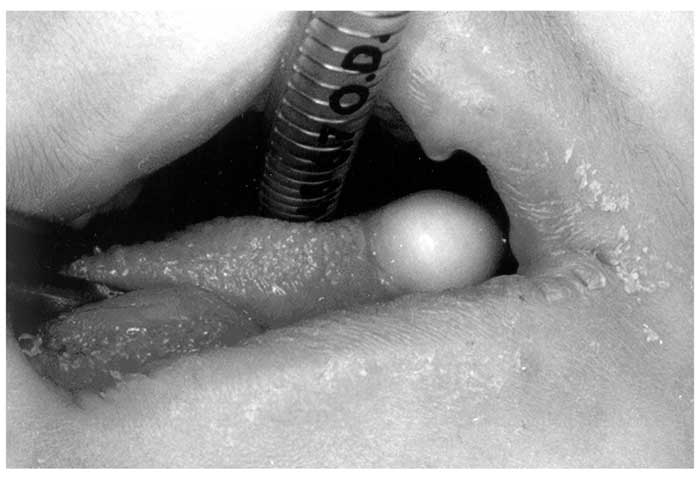
The oral-facial-digital syndrome type 1 is characterized by following abnormalities: pseudocleft of the upper lip, tongue lobulation, hamartomata on the tongue, alveolar frenulae, and clefting of the soft palate. We report a 9-month-old girl who was referred to our clinic due to facial dysmorphology in addition to cleft palate and multiple masses on the tongue which resulted in feeding problems. Surgical intervention was done. Molecular analysis revealed absence of OFD gene. Key words: Feeding disorders of childhood, Mutation analysis, Oral-facial-digital syndrome type 1. Oral-facial-digital syndromes are a heterogeneous group of developmental disorders of which at least nine different forms have been described(1). It is transmitted as an X-linked dominant condition and is characterized by malformations of the face, oral cavity and digits(1-4). The gene for the disorder was mapped to Xp22.3-p22.2(3-7) and mutation analysis identified CXORF5, which was then renamed OFD1 as the gene responsible for this diosorder(5,7). The facial features include frontal bossing, facial asymmetry, hypertelorism, a broadened nasal bridge, and facial milia. Oral features include pseudoclefting of the upper lip, cleft palate and tongue, high arched palate, ankyloglossia together with abnormal dentition. Malformations of the digits of the hands are more common than those of the feet and include syndactyly, brachydactyly, clinodactyly and less commonly polydactyly. In addition poly-cystic kidneys have been found in patients with OFD 1 at necropsy(2). Here we report a child, displaying clinical findings of OFD 1, who was negative for mutations in the OFD 1 gene. Case Report A 9-month-old female was referred for clinical genetic examination because of multiple masses on the tongue, cleft palate and facial dysmorphology. The patient was born to a 30-year-old gravida 1 para 1 mother and a 30- year old father. The parents were healthy and unrelated. Her family history was remarkable: her grandmother’s one brother had severe irregular placement of teeth, another sister and brother’s sister had lobulation of the tongue, and one aunt had partial alopecia on the vertex. Her mother reported to have taken metamizol and eritromysin, for upper respiratory system infection, for one week during the 6-gestational-week. Pregnancy and delivery were normal and her birth weight was 2900 g, length 50 cm. On physical examination, her height, weight, head circumference were 64 cm (50-75th centile), 7800 g (10-25th centile), 42.7 cm (10-25th centile) respectively. She had hypertelorism, depressed nasal bridge, sulcus of the nasal tip, median partial cleft of the upper lip, hyperplastic multiple oral frenuli, cleft palate, bifid, lobulated tongue with multiple hamartoma, milia of ears, partial alopecia on the vertex hair and brachydactyly of all fingers and clinodactyly of the bilateral fifth fingers (Figs. 1 & 2). The left thumb had radial deviation Her mental and motor development, as well as audio-logical examination were normal. She did not have any skeletal anomaly.
Her echocardiography showed third degree mitral valve insufficiency. Cranial magnetic resonance imaging, abdominal and renal ultrasounds were normal. She was operated for cleft palate and hamartoma of tongue. Pathological examination of tongue biopsies showed normal cartilaginous tissue, minor salivary glands and smooth muscle which was reported as "choristoma" on histopathology. It presents as a benign tumor like mass of normal cartilage structure with mature cells in an abnormal position. The karyotype was 46, XX. In order to identify the underlying molecular defect, the 23 coding exons codifying the OFD1 transcript were analyzed. Molecular Analysis Methods: Primers and conditions used for mutation analysis have already been described(3). PCRs were carried out on genomic DNA extracted from peripheral blood leukocytes using the Gentra systems Capture Column Kit. PCR products were checked on agarose gel and used for DHPLC análysis using the Wave DNA fragment analysis system (Transgenomic, Inc.) according to the manufacturer’s instructions. Full ethical approval was obtained for the study. Discussion In order to test the possible involvement of OFD1, we performed molecular analysis of the OFD1 transcript. Our analysis did not reveal abnormalities in the patient when compared to normal controls. Although we cannot exclude the possibility that the patient does carry a mutation in the OFD1 gene which could not be identified by our approach, our data might indicate that the patient may be affected by a different form of OFD for which molecular testing is not yet available. Both OFD 1 and OFD 2 have overlap findings. Pseudocleft of the upper lip, tongue lobulation, hamartomata on the tongue, alveolar frenulae, and clefting of the soft palate and abnormalities of hands and feet are common to both conditions. Alopecia and milia have been reported only in type 1(7). Our patient has common facial findings of OFD 1 in addition to alopecia and milia. A hamartomatous mass on the ventral surface of the tongue is seen in 70% of the cases(7). Our patients’ clinical findings were not in accord with the other types of OFD. However, patients without a pathogenic OFD 1 mutation have low frequently lingual hamartomas (7). We would like to emphasize that any patient with tongue masses and cleft palate associated with feeding problems should be evaluated for OFD 1. Contributors: All authors contributed to case management, review of literature and drafting of the article. Funding: None. Competing interests: None.
|
![]()